When Vaccines Work: Why We Forget the Diseases They Prevent
The sight of an empty hospital ward, a quiet pediatric clinic in summer, or the lack of a feared childhood paralysis is, on its face, the happiest of public-health outcomes. Yet beneath that success there is a quieter, more dangerous phenomenon: the very effectiveness of vaccines erases the visceral memory of what these diseases did. Without the daily evidence of smallpox scars, diphtheria membranes, or polio-crippled limbs, societies can misjudge risk, underinvest in prevention, and become vulnerable to complacency and misinformation. This article traces the paradox of vaccine success — how victory becomes invisibility — and offers ways to keep memory alive while sustaining trust and uptake.
The Paradox Defined
At its core, the paradox is simple: the better a vaccine works, the less people see the problem it solves. That absence of visible harm changes how individuals assess personal risk. When danger is not immediate or visible, human psychology — prone to availability heuristics and optimism bias — favors short-term convenience over long-term protection. Vaccination, which asks a tiny present-month investment (scheduling a clinic visit, tolerating a temporary sore arm) for a diffuse long-term collective benefit, can lose out to inertia.
Availability and Optimism
Behavioral science shows that people judge frequency and severity of events by how easily examples come to mind. If a parent has never seen a child coughing blood from pertussis or lying limp from meningitis, those images cannot anchor their decision-making. Optimism bias — the belief that bad things are less likely to happen to oneself — compounds this. The result is a social environment where vaccination is seen as optional rather than essential.
Collective Forgetting and Storytelling
Memory about diseases is cultural as much as personal. For generations, parents passed stories of disease and loss—grandparents with pitted faces from smallpox or aunties who never walked properly after polio. As those firsthand witnesses vanish from family narratives, the stories fade. Schools reduce time spent on public-health history. Popular media favors new worries over old ones. Without stories, the public’s reservoir of caution runs dry.
History: Proof and Warning
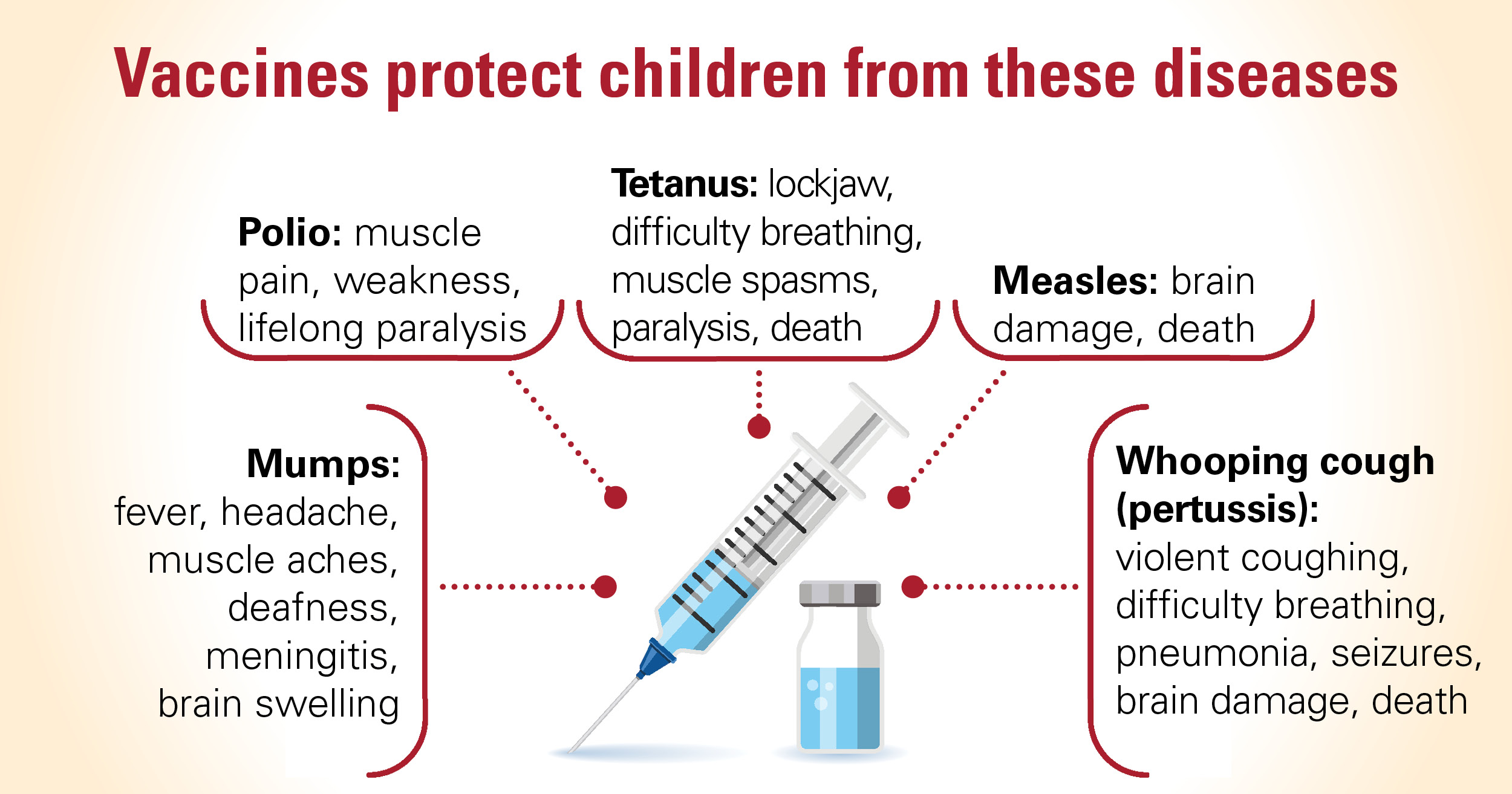
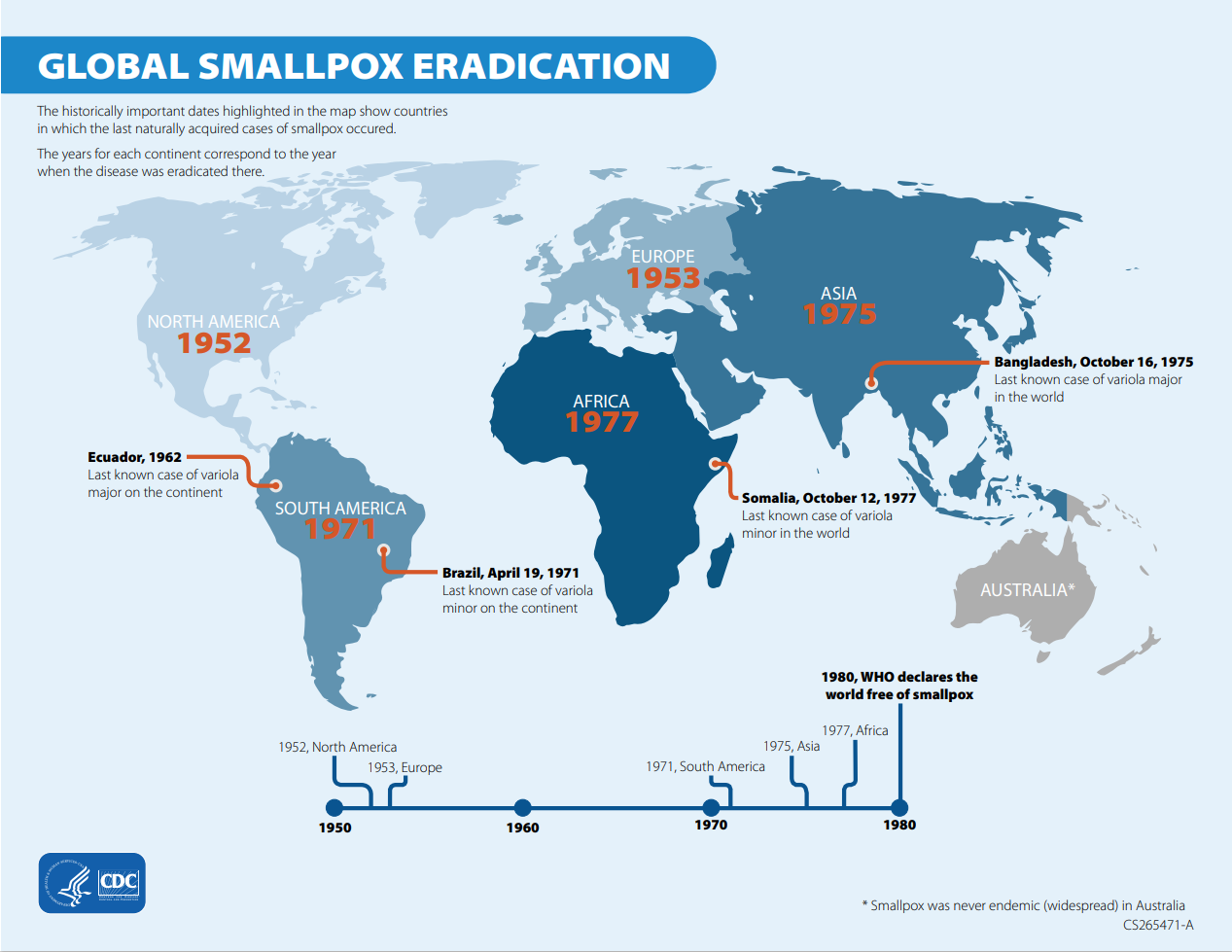
History is the laboratory where this paradox can be seen most clearly. Smallpox, which once killed and disfigured millions, was declared eradicated in 1980 after a coordinated global campaign. Polio, once a household fear, is now restricted to a handful of countries. Measles, once nearly universal in childhood with predictable complications, has become rare in regions with high vaccine coverage. Each success story also subtly rewrites public perception: eradication can make prevention seem permanent rather than maintained.
Caption describing the image
Smallpox — The Ultimate Paradox
Smallpox eradication is both triumph and trap. The world eliminated a disease that had stalked humans for millennia. But because it is gone, new generations have no direct experience of its devastation. When a problem disappears, funding and political will can recede. The smallpox story instructs: eradication requires not just scientific strategy but sustained memory and institutional commitment long after the last case.

Caption describing the image
Polio and the Long Tail
Polio’s near disappearance in many countries created a new category of complacency: the “long tail” problem. When cases drop into the low hundreds or dozens, the public imagines the end is permanent. Yet viruses can linger in under-immunized pockets and travel with human movement. Local declines in vaccination leave openings for reintroduction, as seen in sporadic outbreaks when coverage falters.
Caption describing the image
Consequences of Forgetting
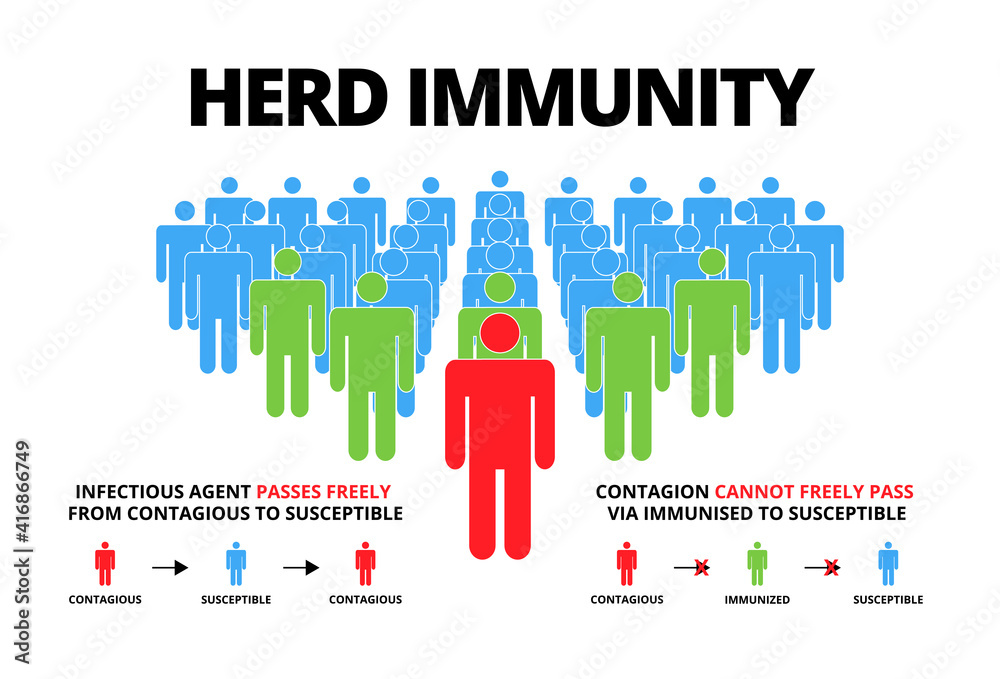
The immediate consequence of forgetting is increased vulnerability. When vaccination coverage moves below thresholds required for herd immunity, outbreaks can re-emerge. But the costs go beyond epidemiology: they reshape policy, funding, and the social contract between science and society.
Caption describing the image
Policy and Funding Erosion
Public health programs are often the first to feel budgetary pressure during fiscal tightening because their success makes their need invisible. When disease incidence is low, lawmakers may redirect funds to problems with clearer immediate returns. This cyclical defunding can leave surveillance and vaccine-delivery infrastructure brittle — precisely the systems required to prevent resurgence.
Rise of Misinformation
When lived experience does not contradict false claims, misinformation spreads more easily. Assertions that vaccines are unnecessary, harmful, or a matter of personal choice resonate when the counter-evidence — a ward full of sick children — is absent. The vacuum created by forgetting is quickly filled by narratives and tropes that require little factual grounding.
Caption describing the image
Psychology and Social Dynamics
Understanding why societies forget requires a look at cognitive, social, and cultural forces. Four dynamics are particularly important: normalization of safety, diffusion of responsibility, changing risk signals, and identity politics.
Normalization of Safety
As vaccines reduce disease, the absence of harm becomes the new normal. Normalization breeds complacency because daily life reinforces the idea that things are safe. Safety becomes background noise until a rare outbreak makes it spectral again.
Diffusion of Responsibility
Vaccination is both an individual act and a public-good behavior. When most people vaccinate, the protective shield around society grows, and individual decisions can feel less consequential. This diffusion of responsibility can lead to free-riding behavior — people relying on others to maintain herd immunity while opting out themselves.
Changing Risk Signals
In a pre-vaccine era, risk presented dramatically and frequently. Now it is statistical, mediated by public-health reports and academic papers. Experts interpret risk with nuance; the public often seeks simple cues. Without visible signals, probabilistic warnings fail to mobilize action.
Identity and Belonging
Vaccination becomes entangled with identity and trust. Where trust in institutions is low, people seek alternative communities that reinforce skepticism. The absence of disease removes a corrective reality-check; social identity can then override empirical evidence.
Public memory is a vaccine’s shadow: the more complete the protection, the dimmer the shadow becomes — until an outbreak casts it again.
Caption describing the image
How Societies Can Remember Without Fear
Preserving memory of vaccine-preventable disease does not mean manufacturing terror. It means embedding accurate history, empathic storytelling, and visible markers of progress into culture and policy so that prevention remains valued.
Integrate History into Education
Curricula can include concise, age-appropriate modules about historical diseases, their human toll, and how vaccines changed outcomes. Personal stories, survivor testimonies, and local histories make the abstract concrete. Teaching the successes of public health alongside scientific method fosters both gratitude and critical thinking.
Humanize the Data
Numbers alone fail to move many people. Pair statistics with human narratives: the parent who lost a child to diphtheria, the community rebuilt after an outbreak, the nurse who traveled to vaccinate remote villages. Such stories create emotional memory without fearmongering.
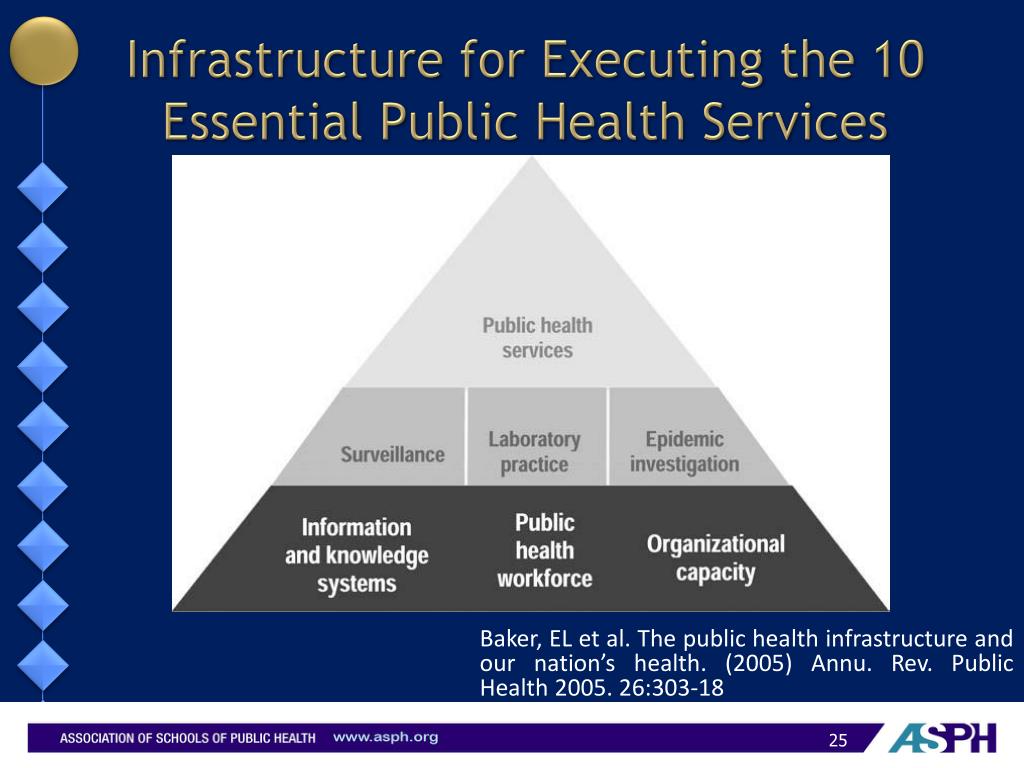
Sustain Visible Infrastructure
Vaccination clinics, memorial plaques, museum exhibits, and public-health anniversaries keep the memory in public space. Visible infrastructure reminds communities that prevention required ongoing effort, and that victory was built — not inevitable.
Transparent Risk Communication
Honest communication about risks and benefits builds trust. Acknowledge side effects, explain rarity, and contextualize risk relative to non-action. When public health speaks plainly and compassionately, it combats misinformation without resorting to scare tactics.
Practical Steps for Policy and Communities
Turning insight into practice requires tools for policymakers, health communicators, and community leaders. The following approaches help maintain high coverage and cultural memory.
Invest in Surveillance and Routine Services
Strong surveillance systems detect declines in coverage early. Routine immunization services should be funded as ongoing civic infrastructure, not crisis commodities. Commitments that appear permanent create steady expectations and normalize vaccination over generations.
Support Community Champions
Local voices — school nurses, religious leaders, trusted clinicians — often persuade more than distant experts. Training and supporting these champions multiplies accurate messaging and keeps memory locally situated.
Leverage Media and Culture
Film, literature, and journalism can preserve public memory. Thoughtful portrayals of outbreaks and the human stakes of prevention, without sensationalism, create durable cultural knowledge. Public-service announcements that recall history in brief, respectful ways can also be effective.
Navigating Ethical Tensions
Remembering disease raises ethical questions: how to maintain memory without exploiting tragedy, how to respect survivors, and how to avoid coercive messaging that undermines trust. Ethical strategies emphasize consent, dignity, and balanced narratives that acknowledge both benefits and risks of public-health action.
Avoiding Fear While Teaching Risk
Facts can be framed to educate rather than frighten. Use proportionate language, avoid hyperbole, and center stories of resilience and recovery as well as loss. Ethics requires that we enlist memory to inform choices, not to manipulate behavior through shame or alarm.
What Individuals Can Do
The paradox of forgetting is not only a governmental problem; individuals contribute to cultural memory. Simple acts can keep awareness alive.
Share Family Histories
Talk to older relatives about illness experiences and pass those stories to younger family members. Personal narratives are exceptional memory anchors.
Model Vaccination as Civic Duty
Make vaccination visible: bring children to clinics, display vaccine cards when appropriate, explain to friends why you chose to vaccinate. Normalizing the practice in social contexts reduces stigma and strengthens norms.
Seek Balanced Information
Prioritize reputable public-health guidance and be wary of anecdote-driven social media claims. Encourage critical thinking and ask questions about sources. Community forums that allow respectful discussion often defuse fear-driven narratives.
Conclusion: Remembering as Prevention
Vaccines gave us something extraordinary: protection that is sometimes invisible and therefore vulnerable. Recognizing that invisibility is not an argument against prevention but a call to stewardship reframes the paradox. Memory — cultural, institutional, and personal — is a public-health tool. When we remember responsibly, we honor the lives saved, sustain the systems that protect us, and reduce the chance that the horrors of the past become tomorrow’s reality.
To preserve health we must preserve memory: not to scare, but to remind that prevention was hard-won and worth keeping.
- Success breeds invisibility: As vaccines reduce disease, public memory fades, altering risk perception.
- Forgetting has costs: Reduced funding, misinformation, and outbreaks can follow declining vigilance.
- Memory is maintainable: Education, storytelling, infrastructure, and transparent communication preserve the lessons of prevention.
- Ethics matter: Teach history without fear, respect survivors, and build trust through honesty.
Final Reflection
Victory over disease is one of humanity’s proudest achievements. The paradox that often follows is entirely human: we are creatures who respond to what we see. If the sight of disease is gone, we must deliberately keep its memory alive — not as a haunt, but as the foundation of a healthier future.