When a Kiss Causes Brain Injury: Preventing Neonatal HSV Encephalitis
Two days after she was born, Breelyn’s family expected only the ordinary new-parent anxieties: feeding, sleep cycles, and the dizzying wonder of a tiny face. They did not expect seizures. They did not expect the ICU alarm lights, the neurologists’ quiet concern, the word encephalitis. A well-meaning visitor had kissed the newborn on the mouth while having a cold sore. The virus that causes a common, usually mild lip lesion—herpes simplex virus—found an unfurnished immune system and invaded the infant’s brain.

Newborn baby seizures ICU
The story of Breelyn is a painful example of a rare but catastrophic event: neonatal herpes simplex virus (HSV) infection leading to encephalitis, seizures, and lasting brain injury. In this article we follow the clinical arc of neonatal HSV encephalitis—how it happens, how it is diagnosed and treated, and, crucially, how it can be prevented. We will also explore what recovery can look like for survivors and how families can navigate the medical, emotional, and practical aftermath.

Cold sore kissing baby
Why newborns are vulnerable
The immune system of a newborn is not a smaller version of an adult's: it is fundamentally different. In the first days of life, maternal antibodies transferred during pregnancy can offer protection against many infections, but that protection is incomplete and patchy. Newborns have immature innate and adaptive immune responses, reduced ability to mount strong inflammatory responses, and less efficient barriers at mucosal surfaces. These factors make infants uniquely susceptible to pathogens that adults usually contain easily.

Hand hygiene newborn baby
HSV types and common presentations
Herpes simplex virus comes in two main types: HSV-1, traditionally associated with oral lesions (cold sores), and HSV-2, more often linked to genital infections. Either type can cause neonatal infection. Transmission routes include passage through an infected birth canal, but postnatal transmission—through direct contact, like a kiss from a person with an active or recently active cold sore—is also a documented and preventable route.
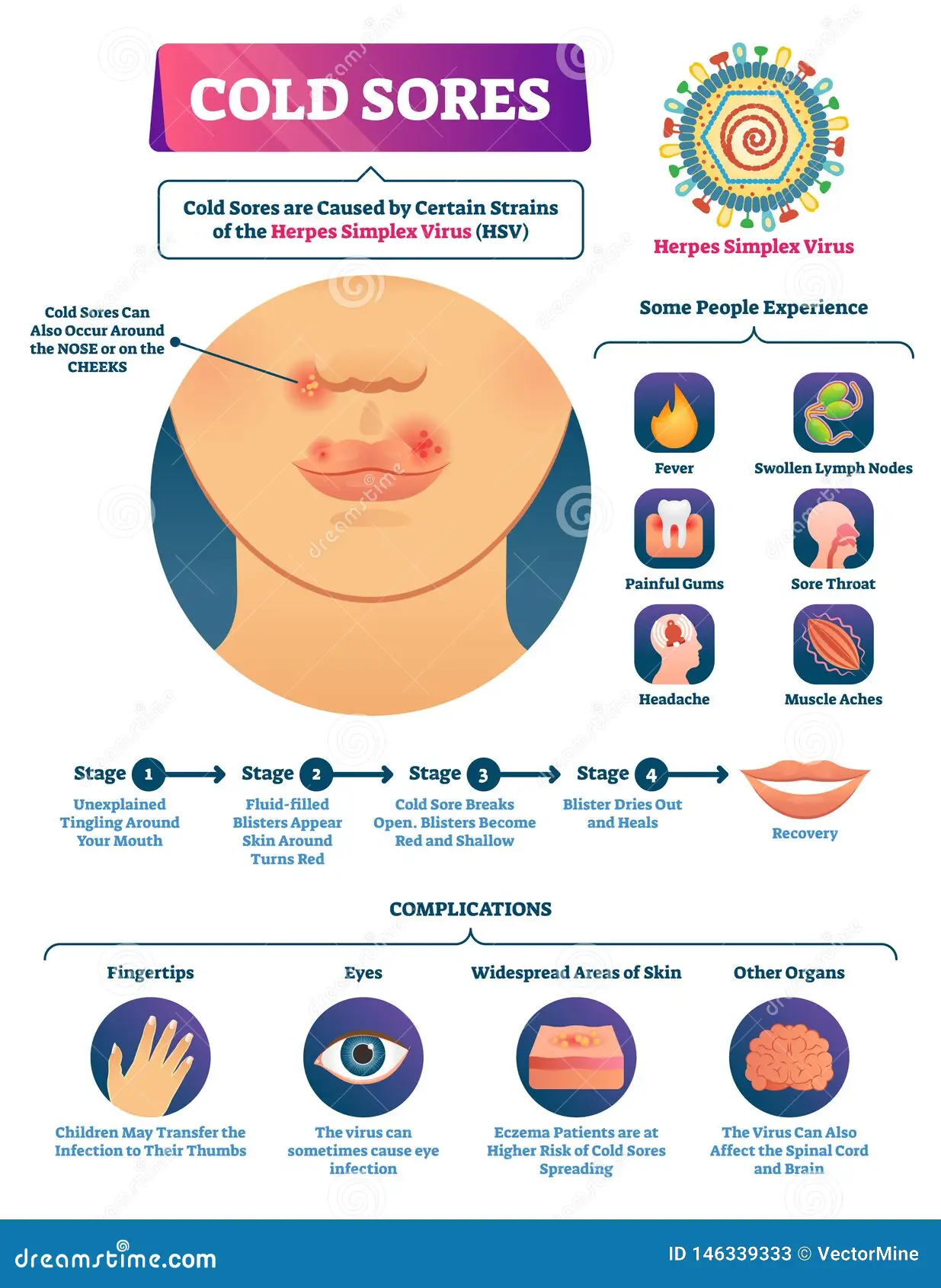
Cold sore virus transmission
A casual kiss can become a medical emergency when an infant's immune system cannot contain a virus adults typically tolerate.
How HSV reaches the infant brain
There are three clinical patterns of neonatal HSV: skin-eye-mouth disease, disseminated disease affecting organs such as the liver and lungs, and central nervous system (CNS) disease—encephalitis. The last is the most feared. HSV can travel along nerve pathways or through the bloodstream to infect brain tissue. Once it reaches the brain, the virus triggers inflammation, cell death, and swelling. The frontal and temporal lobes are often involved, and the resulting injury can produce seizures, altered consciousness, and long-term cognitive and motor deficits.
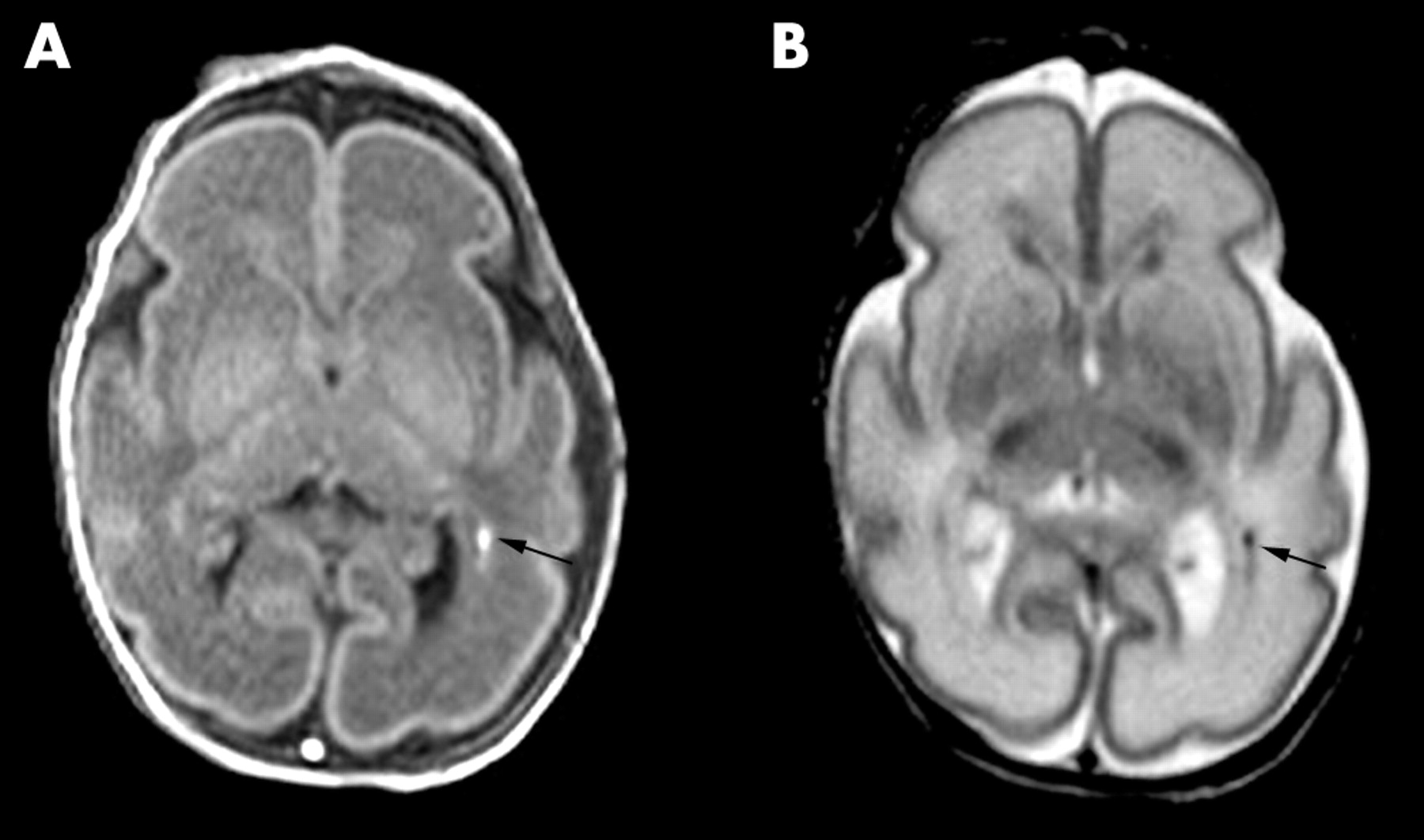
Baby brain injury MRI
Typical clinical course and warning signs
In neonates, symptoms of HSV encephalitis can be subtle at first: poor feeding, irritability, and temperature instability. Within hours to days patients may develop lethargy, decreased responsiveness, breathing difficulties, and most alarmingly, seizures. Because newborn seizures are often brief and may look like unusual movements or staring, they can be missed without a high index of suspicion.
Baby seizure infant care
Red flags for caregivers and clinicians
- Feeding problems: sudden refusal to feed or frequent regurgitation.
- Temperature changes: hypothermia or fever without another clear cause.
- Unusual movements: rhythmic jerking, stiffening, or subtle focal twitching.
- Respiratory distress: apnea or irregular breathing.
- Altered level of consciousness: excessive sleepiness, poor arousal, or unresponsiveness.
Any of these signs in a neonate—especially after a known exposure to a person with a cold sore—should prompt urgent medical evaluation.
NICU baby seizures
Diagnosis: speed matters
Early diagnosis is the single most important determinant in the outcome for neonatal HSV encephalitis. Clinicians rely on a combination of clinical exam and targeted testing. The key tests include lumbar puncture to obtain cerebrospinal fluid (CSF) for HSV polymerase chain reaction (PCR), blood tests for liver function and viral DNA, and brain MRI to evaluate areas of inflammation. Electroencephalography (EEG) helps detect seizures that may not be clinically obvious.
Lumbar puncture infant

HSV PCR testing newborn
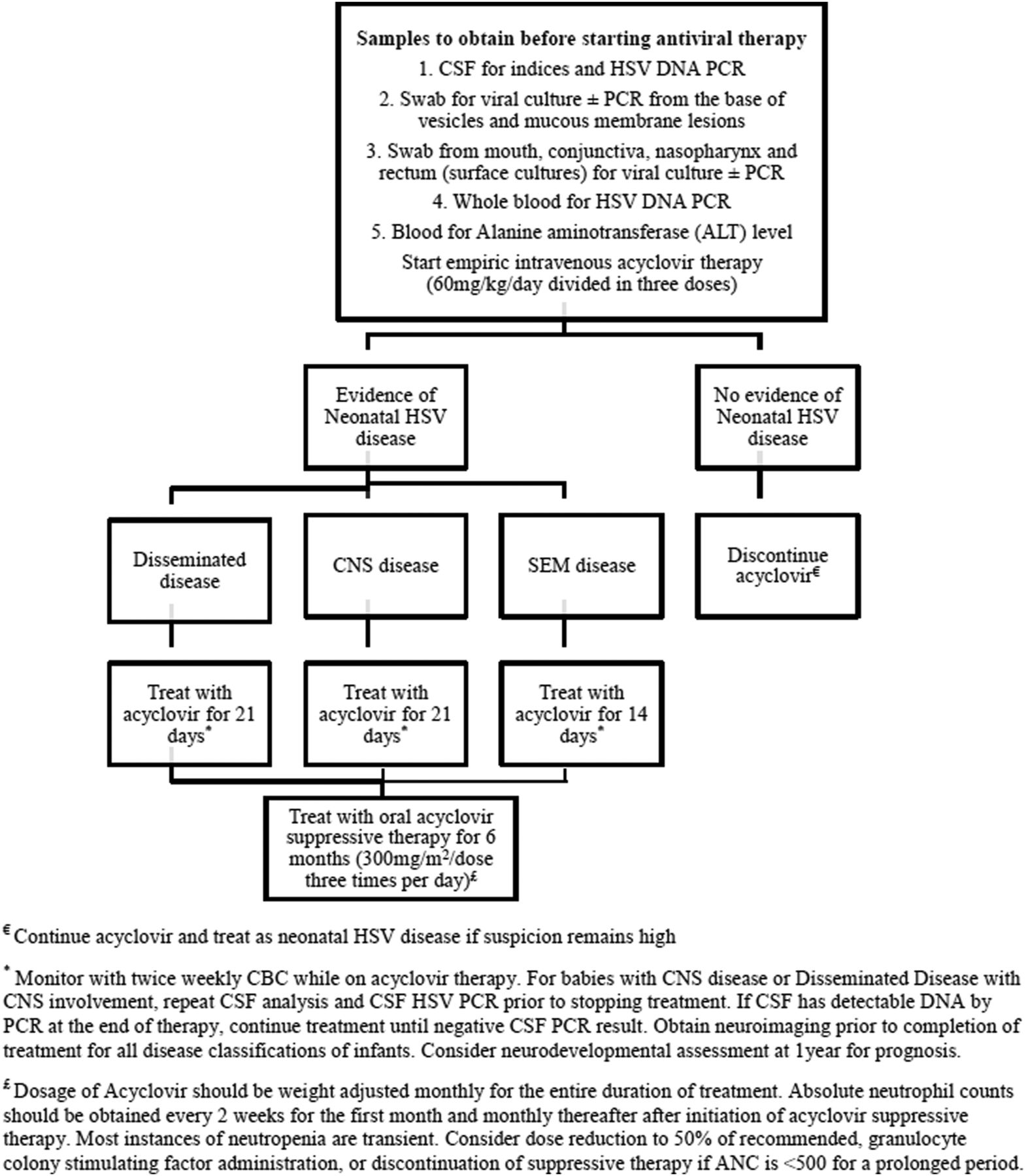
Treatment essentials
High-dose intravenous acyclovir is the standard of care and should be started as soon as HSV encephalitis is suspected. Early antiviral therapy reduces mortality and improves neurological outcomes, although many infants still experience long-term complications. Supportive care in a neonatal intensive care unit (NICU) typically includes seizure control with antiepileptic medications, respiratory support if needed, fluid and electrolyte management, and monitoring for complications such as increased intracranial pressure.

Acyclovir IV vial
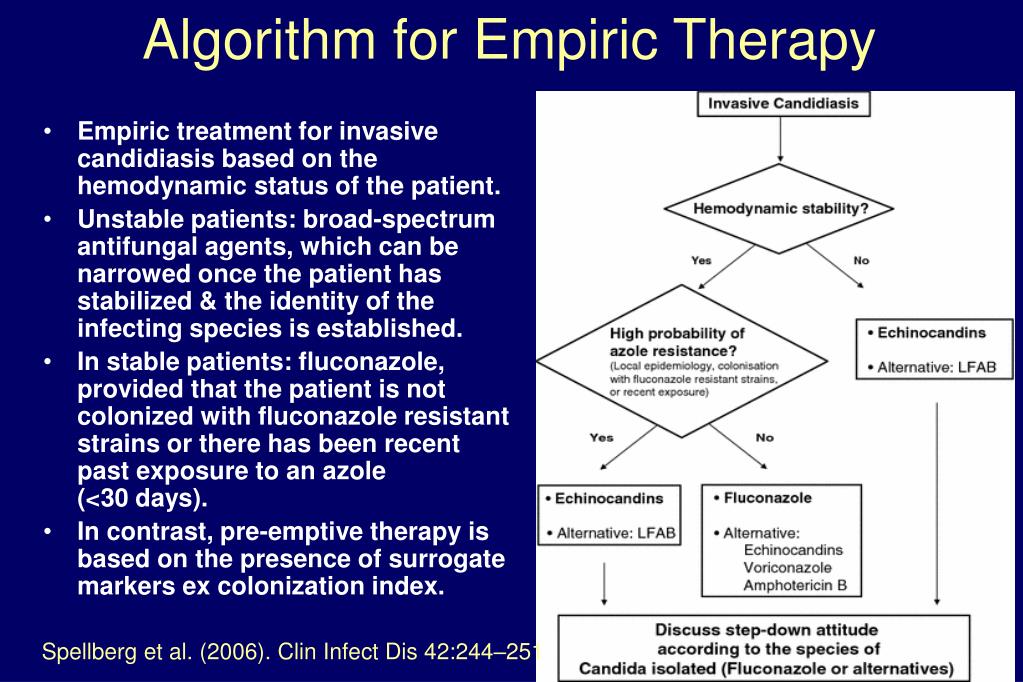
Empiric acyclovir therapy
Prognosis and long-term outcomes
Even with prompt treatment, HSV encephalitis in newborns carries significant risk. Outcomes range from complete recovery to severe, permanent neurological impairment depending on factors such as the timing of therapy, the extent of brain involvement, and the presence of disseminated infection. Common long-term issues include epilepsy, developmental delay, motor impairment, cognitive deficits, and hearing or vision problems. Rehabilitation—physical, occupational, speech therapy, and educational interventions—becomes central to maximizing a child's potential.
Preventing neonatal HSV: practical steps
Because the consequences can be so severe, prevention is paramount. Many measures are simple behavioral changes that protect a newborn without causing fear or isolation.
Actions for parents, family, and visitors
- Do not kiss newborns on the mouth. If you have a cold sore or recently had one, avoid close facial contact until fully healed.
- Maintain strict hand hygiene. Wash hands before holding or feeding the baby, especially after touching your own face or applying creams to a lesion.
- Avoid sharing utensils, cups, or lip products around infants.
- Keep visitors with active sores away from the baby or limit contact to non-face areas until lesions resolve.
Maternal health and delivery planning
Pregnant people are screened and managed when genital herpes is known or suspected. If active genital lesions or prodromal symptoms occur at delivery, cesarean delivery is often recommended to reduce the risk of intrapartum transmission. However, many neonatal HSV infections are postnatal or occur after an asymptomatic maternal infection, so birth planning alone cannot eliminate risk.
What clinicians and hospitals can do
Hospitals can adopt clear visitor policies in maternity wards: educational signage, guidance for staff to screen guests with visible cold sores, and routine counseling for new parents about avoidance of direct mouth contact. Clinicians should maintain a low threshold for testing infants with concerning symptoms and start empiric antiviral therapy when indicated.
Life after encephalitis: supporting families
Recovery is rarely a single moment; it is a process that involves medical milestones and emotional reckonings. Parents of affected infants often confront guilt, anger, and grief over the loss of an expected 'normal' start. Practical supports—clear medical explanations, care coordination, counseling, and connection to other families—help immensely.
Rehabilitation and developmental follow-up
Early intervention services are time-sensitive. Physical therapy addresses motor delays, occupational therapy helps with daily skills, speech therapy supports feeding and language development, and neurodevelopmental pediatricians track cognitive progress. Seizure management may be long-term; some children can be weaned off medications, while others will need ongoing neurology care.
Public health and education
Stories like Breelyn’s are painful but also teachable. Public health campaigns that normalize simple protective behaviors—don’t kiss newborns on or near the mouth if you have a cold sore, wash hands before handling a baby—can reduce risk without stigmatizing people who carry HSV. Education should reach family members, in-laws, and friends as well as new parents.
Addressing common questions
Is there a vaccine?
As of now there is no approved vaccine that prevents HSV infection for widespread use. Research continues, but prevention relies on behavior, clinical vigilance, and targeted maternal management.
Can breastfeeding transmit HSV?
Transmission via breast milk is uncommon. The primary concern is direct contact between an infant's mouth and an active lesion on the breast. If there are lesions on the breast, temporary avoidance paired with expressed milk management and clinician guidance is recommended.
A note on blame and healing
When a loved one's momentary lapse—an affectionate kiss—triggers a medical crisis, blame naturally follows. But prevention education and compassionate support are more useful than recrimination. Parents and families must be given clear, non-shaming information and pathways to care so they can protect infants without turning every interaction into anxiety.
Conclusion
Breelyn’s case is a heartbreaking reminder that commonplace infections can become catastrophic in the context of a newborn’s immature immune system. The path from a cold sore to seizures and brain injury is preventable in many cases through simple measures: don’t kiss babies on the mouth, prioritize hand hygiene, educate visitors, and maintain a high index of suspicion for early warning signs. For clinicians, rapid diagnosis and immediate antiviral treatment are critical.
Prevention requires culture change as much as clinical care: respectful, routine guidance to families and visitors—delivered before a newborn leaves the hospital—can reduce risk. For families already affected, the medical journey is a marathon that blends acute care, rehabilitation, and psychological healing. With early intervention, many children make meaningful progress; with continued support, families find ways to adapt, advocate, and build rich lives for their children.
- Simple actions save lives: avoid mouth-to-mouth contact and practice hand hygiene around newborns.
- Act quickly: early recognition and IV acyclovir markedly improve outcomes for suspected neonatal HSV encephalitis.
- Survivors need long-term support: coordinated rehabilitation and developmental follow-up are essential.
Breelyn’s story underscores the fragile balance between everyday affection and infant safety—and the power of prevention.