Vitamin B12 Deficiency: The Hidden Cause of Aging Symptoms
It arrives slowly: waking up tired, misplacing keys more often, feeling a little light-headed when you stand up, or walking as if your feet don't always get the memo from your brain. Those small changes are easy to chalk up to "getting older." But for many people, the culprit behind these shifts is not inevitable aging at all—it's a common, treatable nutrient deficiency: vitamin B12 deficiency. Left unrecognized, it can erode energy, mood, memory, and balance. Caught early, many effects are reversible.
Why This Matters
Clinicians and patients alike often miss B12 deficiency because its signs overlap with normal age-related complaints. That error matters. Symptoms that look like mild cognitive decline, depression, or peripheral neuropathy may respond dramatically to simple treatment. In a health system that prizes disease prevention and maintaining independence, recognizing B12 deficiency is a low-cost, high-impact intervention—particularly for older adults and people with specific risk factors.
If memory slips, numbness, or fatigue feel like part of aging, ask your clinician about a B12 check—many people improve after treatment.
What Is Vitamin B12 and Why Do We Need It?
The role of B12 in the body
Vitamin B12, also called cobalamin, is a water-soluble vitamin that plays essential roles in red blood cell formation, DNA synthesis, and nervous system maintenance. It helps convert homocysteine to methionine—a reaction central to brain function and cell repair—and it prevents buildup of methylmalonic acid, a byproduct that can harm nerve tissue when left unchecked. Because the body stores B12 in the liver, deficiency can appear slowly, sometimes years after dietary intake decreases or absorption problems begin.
Vitamin B12 molecule structure
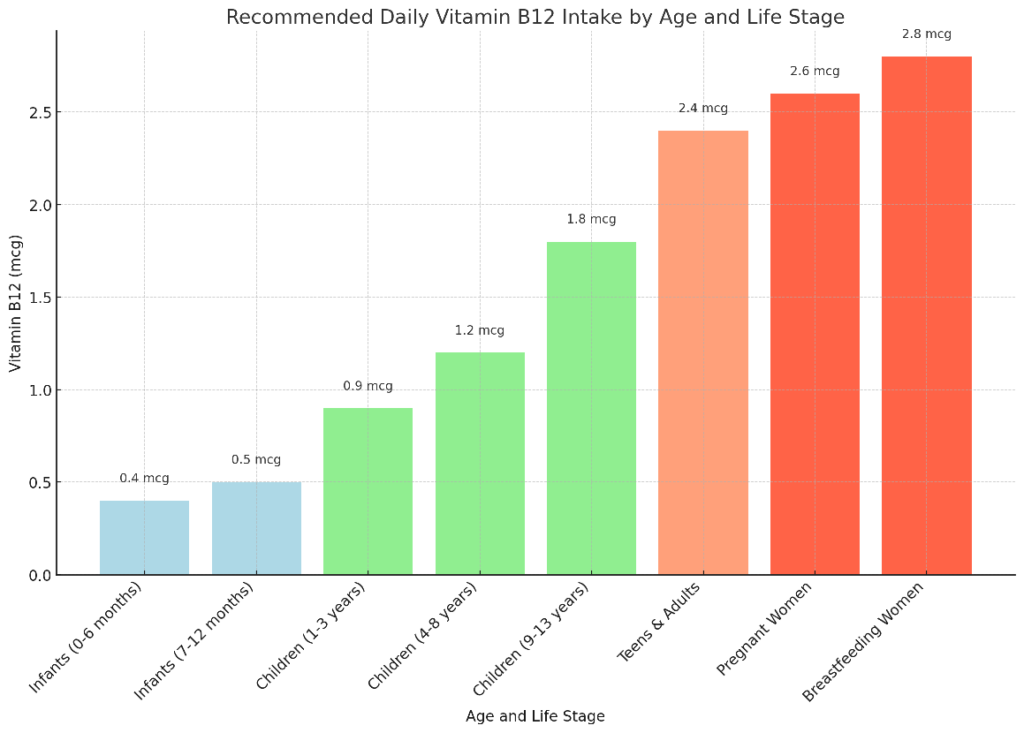
Sources and absorption
Dietary B12 is found naturally in animal products—meat, fish, dairy, and eggs—and in fortified foods. Absorption is a two-stage process: stomach acid releases B12 from food proteins, then intrinsic factor, a protein produced by stomach cells, binds B12 and allows uptake in the small intestine. Disruption at any point—low stomach acid, lack of intrinsic factor, intestinal disease, certain medications—reduces absorption and raises the risk of deficiency.
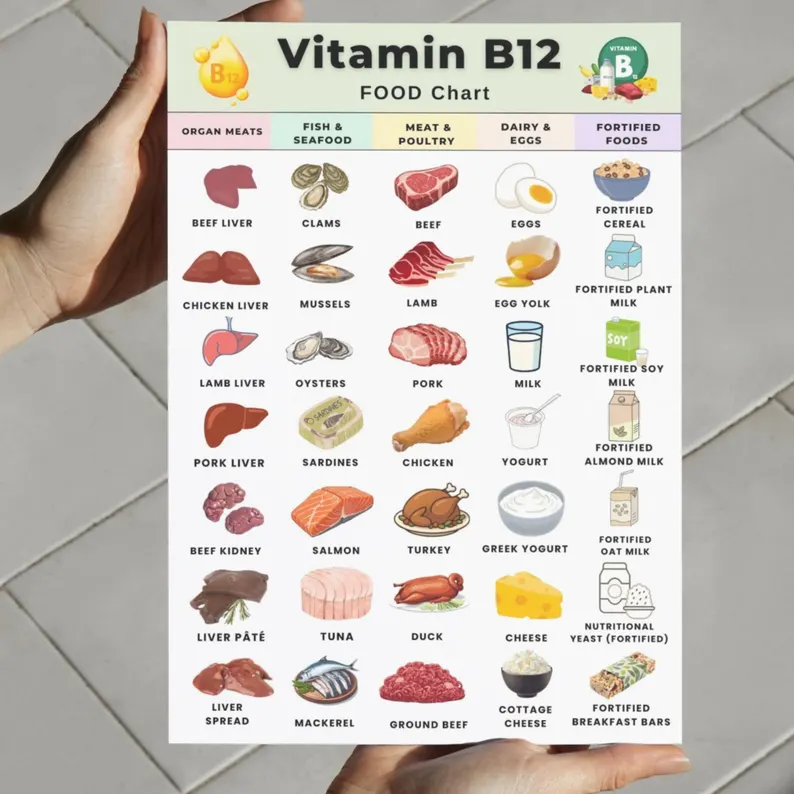
B12 food sources meat fish
Why B12 Deficiency Looks Like Aging
Shared symptoms with aging
Many symptoms commonly attributed to aging are also classic signs of B12 deficiency. These include:
- Fatigue and low energy that aren't explained by sleep quality alone.
- Memory complaints and slowed thinking—difficulty finding words, short-term memory lapses, or "brain fog."
- Balance problems and unsteady gait, which may increase fall risk.
- Numbness, tingling, or burning in hands and feet from peripheral neuropathy.
- Mood changes such as depression, irritability, or apathy.
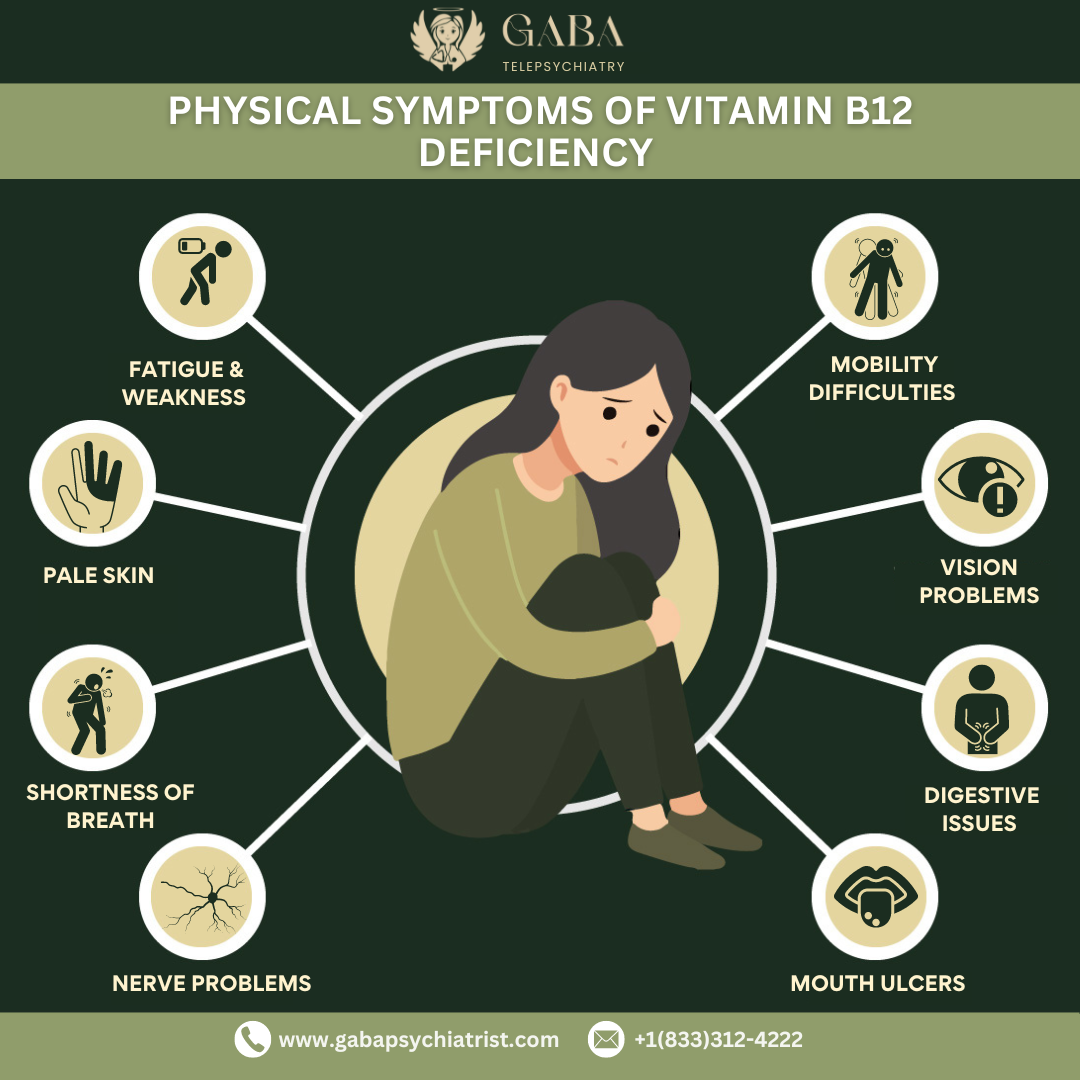
B12 deficiency fatigue symptoms
Because those issues are common in later life, the underlying reversible cause can be overlooked. Unlike some irreversible neurodegenerative conditions, however, early B12-related nerve dysfunction often improves with treatment—especially if recognized before severe damage occurs.
Atypical or subtle presentations
Not everyone develops obvious anemia. Sometimes neurologic symptoms appear with only mild changes on routine blood work. That means a normal-looking complete blood count does not rule out deficiency. Subtle signs—slower walking speed, mild short-term memory changes, unusual fatigue—should prompt clinicians to consider B12 testing, especially in at-risk people.
Who Is at Risk?
Groups with higher likelihood of deficiency
Risk increases with certain diets, medical conditions, medications, and age. Common risk groups include:
- Older adults. Changes in stomach physiology—less acid, atrophic gastritis—reduce B12 release from food.
- People on long-term acid-suppressing medications such as proton pump inhibitors or H2 blockers, which can interfere with absorption.
- People taking metformin for diabetes, which is associated with lower B12 levels over time.
- Vegetarians and especially vegans who do not consume animal products and rely only on fortified foods or supplements.
- People with autoimmune conditions like pernicious anemia, where intrinsic factor is lost due to immune attack.
- Those with intestinal surgery or disorders (e.g., celiac disease, Crohn's, gastric bypass) that affect absorption.
Understanding risk helps clinicians decide when to test and helps individuals prioritize preventive measures.
Did You Know? The body stores several years' worth of vitamin B12, so deficiency often develops gradually—symptoms can be subtle for a long time before becoming obvious.
How B12 Deficiency Is Diagnosed
Clinical evaluation
Diagnosis begins with a careful history and exam: dietary habits, medications, surgical history, and neurologic symptoms. Clinicians specifically ask about tingling, balance, memory changes, mood, and bowel or appetite problems. A neurologic exam will assess vibration sense, reflexes, gait, and coordination.
Blood tests that matter
Common tests include a complete blood count (CBC) and serum B12 level. But there are pitfalls: a borderline or "normal" serum B12 does not guarantee adequate function. More specific tests—serum methylmalonic acid (MMA) and homocysteine—rise when B12-dependent reactions fail and are more sensitive indicators of deficiency. Testing for intrinsic factor antibodies helps identify pernicious anemia. Clinicians use the total picture—symptoms plus targeted labs—to decide on treatment.
B12 blood test vial
Caution A normal CBC or serum B12 does not rule out deficiency. If symptoms point to B12 problems, ask about MMA or homocysteine testing.
Treatment: What Works
Replenishing B12
Treatment aims to quickly correct the deficiency and then maintain adequate levels. Options include high-dose oral supplements and intramuscular injections. Traditional practice favored injections—especially for people with absorption problems—but research shows that high-dose oral therapy (for example, h1,000–2,000 micrograms daily) can be effective because a small percentage of B12 is absorbed passively even without intrinsic factor. Choice depends on severity, underlying cause, and patient preference.

Vitamin B12 injection treatment
Typical regimens
Regimens vary: severe neurologic symptoms often prompt initial injections—commonly monthly after a rapid loading phase—followed by maintenance therapy. For dietary deficiency without absorption issues, daily oral supplementation or regular fortified foods may suffice. Treatment should be individualized, with follow-up testing (serum B12, MMA) and clinical reassessment to ensure improvement.
Prevention and Practical Steps
Dietary strategies
People who eat animal products typically get enough B12 from food; those who do not should choose fortified cereals, plant milks, or reliable supplements. Reading labels and choosing fortified items with an adequate percentage of daily value matters. For older adults, simply increasing dietary intake may not be enough if absorption is impaired—screening and supplementation become more important.

B12 supplement pills bottle
Medication review and risk mitigation
Review medications with a clinician or pharmacist. Long-term proton pump inhibitor use and metformin are manageable risks: clinicians can consider dose adjustments, monitoring, or supplementation rather than abrupt discontinuation of essential drugs. For people with gastric surgeries or pernicious anemia, a plan for ongoing replacement—often lifelong—should be established.
Important Don't stop or change prescribed medicines without talking to your clinician. Instead, ask whether B12 monitoring or supplements are recommended while you continue the drug.
When to See a Doctor
Red flags
If you experience any of the following, seek evaluation:
- New or progressive numbness or weakness in limbs.
- Sudden or worsening memory problems or confusion.
- Difficulty walking or frequent falls.
- Persistent fatigue that interferes with daily life despite good sleep.
Early medical review can prevent progression to irreversible nerve damage and clarify whether symptoms stem from B12 deficiency or another condition.
Common Questions and Myths
Myth: B12 only causes anemia
Reality: While B12 is critical for red blood cell production, neurologic symptoms can occur without significant anemia. That's why relying solely on hemoglobin or MCV to screen for deficiency misses cases.
Myth: Supplements always fix it
Reality: Supplements help most people, but when absorption is severely impaired—such as pernicious anemia or after certain gastric surgeries—intramuscular injections may be the most reliable option. Follow-up testing and clinical monitoring guide long-term strategy.
A Practical Checklist You Can Use
Use this checklist before your next primary care visit to focus the conversation:
- List symptoms: fatigue, numbness, memory problems, mood changes, balance issues.
- Note medications: long-term PPIs, metformin, recent antibiotics, or other chronic drugs.
- Review diet: vegetarian/vegan, limited animal foods, reliance on processed meals.
- Past medical history: gastric surgery, autoimmune disease, intestinal disorders.
- Ask specific tests: serum B12, methylmalonic acid (MMA), homocysteine, CBC, intrinsic factor antibodies if autoimmune risk.
Real-World Impact: Stories and Outcomes
Clinicians often share anecdotes: an older patient labeled as having "mild cognitive impairment" who regained clarity after B12 treatment; a person with months of numbness who stopped falling and felt more energetic after therapy. These stories underscore an important point: some conditions that appear chronic and progressive are, in fact, treatable when the right cause is identified.
Improve functionMany people see measurable gains in energy, balance, or mood within weeks of treatment when deficiency is the cause.
Conclusion: Don't Accept "Just Getting Older" as the Whole Story
Age changes physiology, but not every symptom that arrives in midlife or later is an unavoidable consequence of time. Vitamin B12 deficiency is common, often underdiagnosed, and frequently reversible. By staying curious—about diet, medications, and subtle neurologic signs—patients and clinicians can find opportunities to restore function and quality of life.
- Vitamin B12 deficiency can mimic normal aging with fatigue, memory problems, neuropathy, and balance issues.
- Risk groups include older adults, vegans, people on long-term PPIs or metformin, and those with certain gastrointestinal conditions.
- Diagnosis may require more than a serum B12 level; MMA and homocysteine are useful when suspicion is high.
- Treatment—oral high-dose supplements or injections—often improves symptoms, especially when started early.
- Bring a focused symptom and medication list to your clinician and ask about B12 testing if you or a loved one are experiencing concerning changes.
Final note
Simple tests and treatments can change trajectories. If subtle declines in energy, mood, memory, or mobility have crept into your life or the life of someone you care for, consider whether vitamin B12 deficiency could be part of the picture. It's a small change that, for many people, makes a big difference.