When Visual Snow Stopped Being Rare
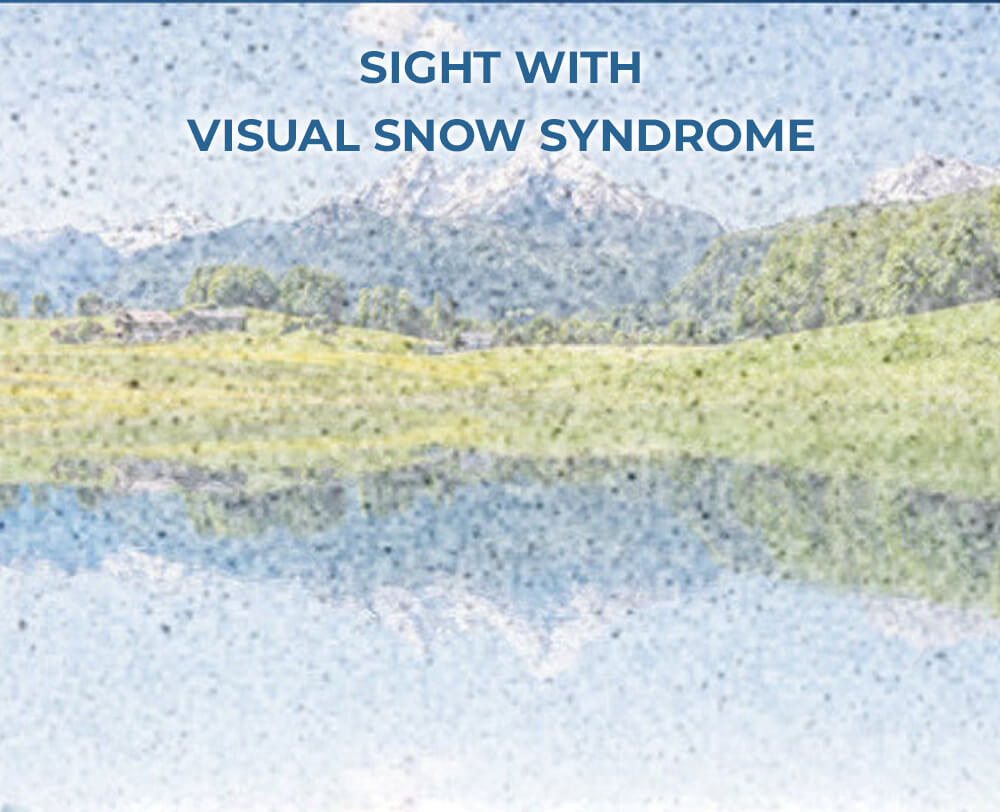
The first person I spoke with described it like watching an old television set that had never been unplugged: a faint, constant frost across the field of vision, present in bright rooms and dim ones, in the sky and on a blank wall. For decades such descriptions were filed as curiosities or misperceptions — part of a patient's vague complaint dismissed in a twenty-minute clinic slot. But in recent years, the chorus grew louder. Patients compared stories on forums, described identical patterns to clinicians, and the phenomenon began to shed the cloak of rarity. What changed was not a sudden spike in biology; it was the simple act of recognition.
visual snow syndrome static
THE MOMENT OF RECOGNITION
Recognition is a small social miracle. When one person says aloud what they have always assumed was unique, others realize two things: they are not alone, and their experience can be described with words that other people understand. For visual snow — a persistent visual static that can overlay everything someone sees — that moment of recognition often starts online. Forums, social media threads, and patient-run websites have allowed people to compare symptoms, co-occurring conditions, and triggers. The language of visual snow crystallized: static, snow, flicker, blue field entoptic phenomenon, and afterimages became part of a shared vocabulary. Once a shared vocabulary exists, clinicians and researchers listen differently.

patient online support groups
Why recognition matters
Recognition transforms clinical data. A symptom seen as idiosyncratic disappears into a pattern once enough people report it. Medical literature historically lags behind lived experience; case reports and small series accumulate slowly, and conditions that are atypical or difficult to quantify remain under-studied. When patients organize, they accelerate detection and research. They propose diagnostic criteria, fund pilot studies, and demand that neurologists and ophthalmologists take a second look.
WHAT IS VISUAL SNOW?
At its simplest, visual snow is the subjective perception of tiny flickering dots across the entire visual field, like the static between channels on a television. Unlike floaters, which move with eye motion and cast shadows, visual snow is usually described as a continuous, fine-grain overlay that can persist for years. It is often accompanied by other visual symptoms — afterimages, trailing of moving objects, light sensitivity, and difficulty seeing at night. Clinicians use the term "visual snow syndrome" when this constellation of symptoms becomes chronic and debilitating for the person affected.
cortical hyperexcitability brain
How patients describe it
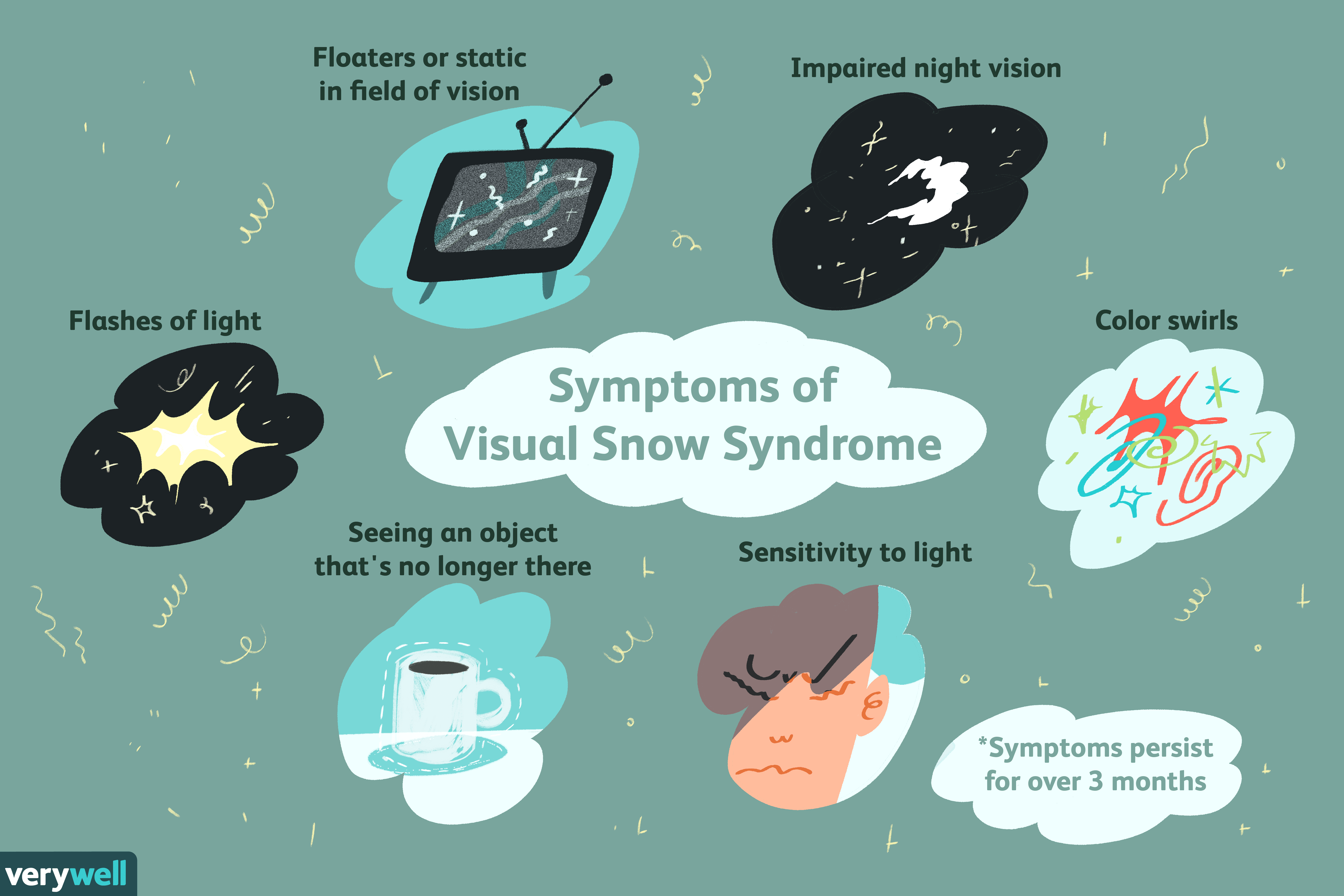
Descriptions vary, but common reports include:
- Static or "snow" covering the whole visual field, sometimes described as black-and-white, sometimes as colored dots.
- Palinopsia, or persistent afterimages and trailing of moving objects.
- Photophobia or a heightened sensitivity to light.
- Blue field entoptic phenomenon, noticing tiny moving dots that are actually white blood cell shadows in the capillaries — but in visual snow the experience is more pervasive.
A HISTORY OF MISUNDERSTANDING
For decades, patients who reported these symptoms were told their vision was structurally normal and that the problem was likely psychological. That dismissal is not always malicious — early ophthalmologic exams often are normal because visual snow arises from processing differences in the brain rather than a damaged eye. Still, the practical effect was a long diagnostic odyssey for many. Some were shuffled between optometrists, ophthalmologists, and psychiatrists. Others were told their complaints were stress-related or manifestations of anxiety.
That narrative began to shift as neurologists noticed overlaps with migraine and as small case series established a reproducible symptom cluster. The modern concept of visual snow syndrome emerged when clinicians recognized that the symptom set could not be explained away by routine imaging or ophthalmic tests alone. Instead, evidence pointed toward a disorder of cortical processing — the brain receiving and handling visual information differently.

tinted lenses visual snow
WHAT SCIENCE THINKS IS HAPPENING
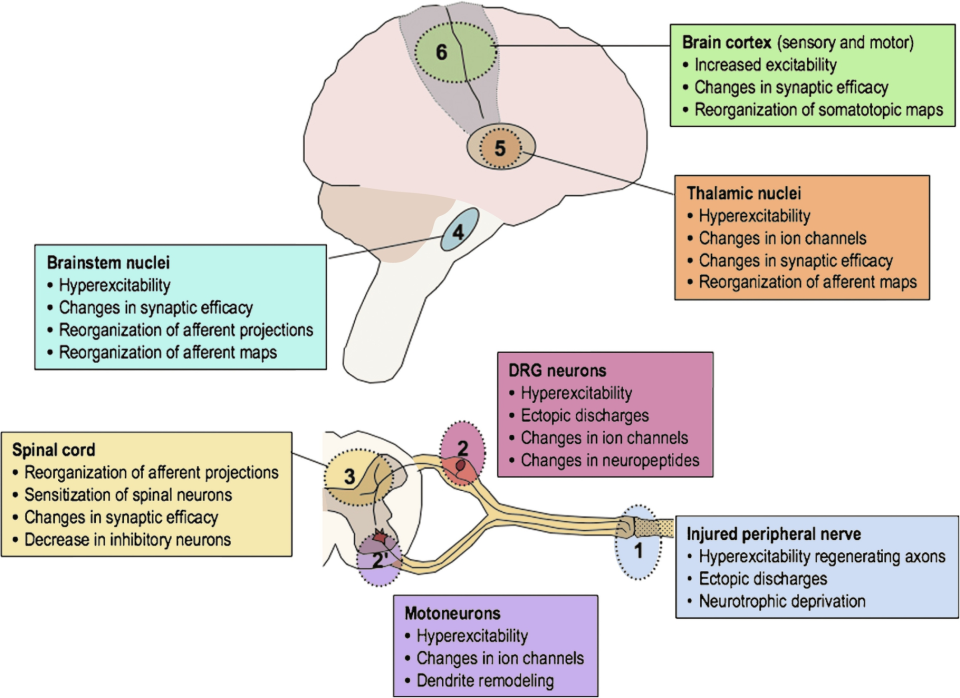
The consensus is incomplete but converging. Several hypotheses have traction:
- Cortical hyperexcitability: sensory neurons in visual cortex may be more easily activated, producing spontaneous visual noise.
- Thalamocortical dysrhythmia: altered rhythms between the thalamus and cortex that change how sensory information is filtered.
- Impaired visual gain control: the mechanisms that suppress irrelevant background information may be less effective, so the brain can't quiet down minor visual signals.
These ideas are not mutually exclusive. Functional imaging studies have shown differences in visual cortex activity in people with visual snow, and electrophysiology suggests abnormal cortical responses to visual stimuli. At the same time, routine MRI scans are usually normal, which is why many patients encountered skepticism before recent research gained momentum.

neurology clinic consultation
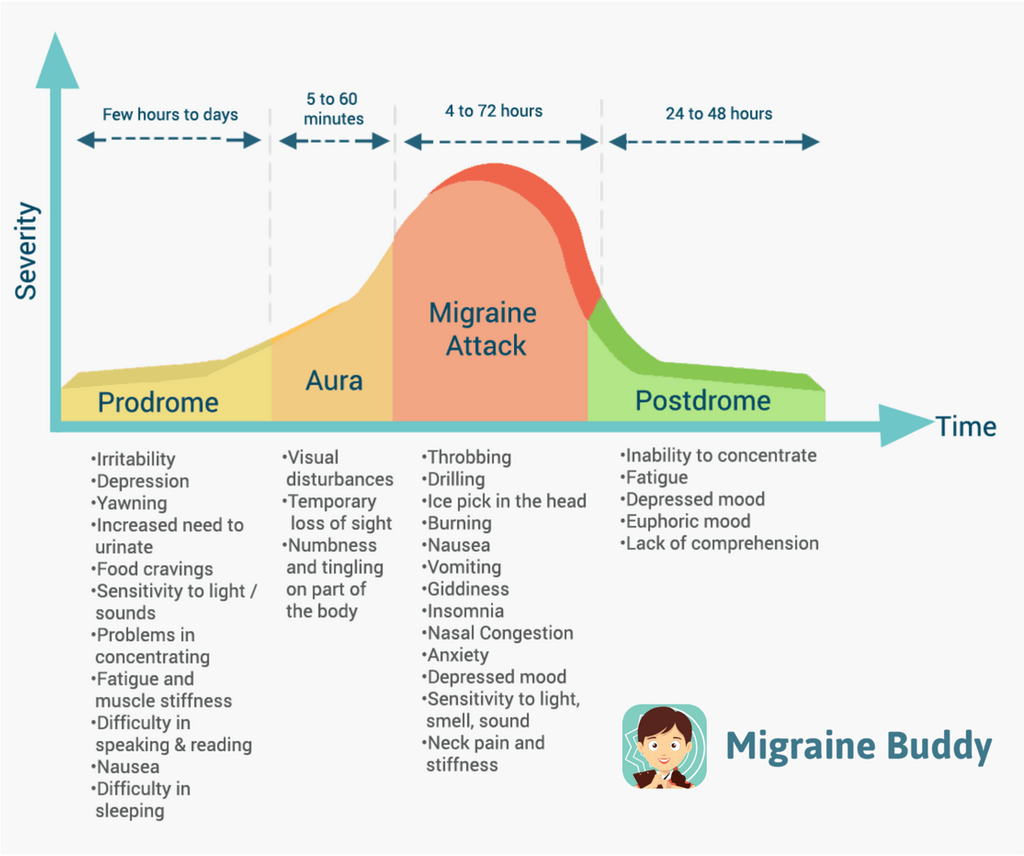
Links to migraine and other comorbidities
One of the clearest epidemiological clues is the high rate of migraine among people with visual snow. Migraines, especially those with aura, share features—sensitivity to light, transient visual disturbances—and possibly neural mechanisms with visual snow. Tinnitus (a persistent ringing in the ears) is another common co-occurrence, suggesting a generalized sensory processing alteration rather than a problem confined to vision alone.
migraine aura comorbidity
HOW COMMON IS IT?
Estimating prevalence is challenging. If clinicians never ask and patients never report, the condition is easy to miss. A growing number of population-based surveys and clinical series suggest visual snow is more common than once believed, though by no means universal. Some studies indicate that a small but significant percentage of the general population experiences symptoms consistent with visual snow at some point, but only a fraction of those people find it disruptive enough to seek care. The truth likely sits between "extremely rare" and "common" — a spectrum where awareness and severity determine who gets counted.
THE PATIENT EXPERIENCE
Beyond clinical definitions, the lived experience matters most. For some, visual snow is a minor annoyance; for others, it erodes concentration, undermines driving confidence, worsens sleep, and increases the emotional burden of everyday life. The constant presence of visual noise can create feelings of alienation: how do you explain a persistent, invisible overlay of the world to coworkers, family, or doctors? Community spaces became an explanation shortcut. When patients discovered online communities, they found validation, practical tips, and sometimes referrals to sympathetic clinicians.

brain imaging visual cortex
Coping strategies people try
There is no one-size-fits-all fix, but patients and clinicians have compiled strategies that help some people reduce distress:
- Tinted lenses or precision tints that reduce contrast sensitivity and may lessen perceived static.
- Screen adjustments like reducing brightness, increasing font size, and using blue-light filters.
- Behavioral strategies including stress reduction, sleep hygiene, and paced visual tasks to avoid fatigue.
- Medication trials guided by a neurologist, sometimes including migraine preventives or off-label neuromodulators, though responses are variable.
WHERE MEDICINE STANDS NOW
Clinicians now recognize visual snow as a legitimate syndrome. Consensus statements have started to define diagnostic criteria based on symptom clusters and duration. That recognition has consequences: insurance becomes easier to navigate when a condition has diagnostic criteria; researchers can design clinical trials with clearer inclusion rules; and trainees learn to ask the right questions during history-taking.
Yet many gaps remain. There is no definitive cure, and treatments are largely symptomatic. Basic research into mechanisms is accelerating but remains limited by funding and the heterogeneity of patient presentations. Still, the shift from dismissal to inquiry is profound: patients who once left clinics uncertain now leave with validation and a plan, even if the plan is tentative.
THE ROLE OF PATIENT COMMUNITIES
One of the clearest lessons from the rise in visual snow awareness is the power of organized patients. Online platforms served as incubators: symptom lists were refined, anecdotal treatments were tested, and the more persistent stories found clinical partners. Patients contributed to study recruitment, funded preliminary research, and pressed publishers and conferences to take notice. This combination of activism and collective data turned isolated case reports into patterns demanding explanation.
What clinicians learned from listening
Clinicians who engaged with patient networks discovered practical insights that textbooks lacked. Details like onset patterns, daily variability, and subtle triggers became visible only when aggregated across many accounts. Those insights informed study design and changed the questions asked during neurological exams. Listening turned a nebulous complaint into a definable research problem.
POTENTIAL FUTURE DIRECTIONS
Where might science and care go next? Several plausible paths appear:
- Targeted neuromodulation: noninvasive brain stimulation methods that adjust cortical excitability in targeted regions.
- Precision optics: refined lenses or adaptive technology that reduce cortical demand for visual processing.
- Pharmacological trials: medications that modulate thalamocortical rhythms or neurotransmitter balance, tested in randomized controlled trials.
- Large-scale epidemiology: population studies to clarify prevalence, risk factors, and natural history.
Each path requires rigorous study design and patient partnership. The patients who helped define the syndrome are the same people who can maximize the impact of future trials by enrolling, advising, and sharing outcome priorities.
PRACTICAL ADVICE FOR THOSE LIVING WITH VISUAL SNOW
If you are reading this because you or someone you love experiences persistent visual static, here are practical steps to consider:
- Document symptoms: keep a diary of onset, triggers, and associated symptoms like headache or tinnitus.
- Seek a thorough exam: start with a neuro-ophthalmologist or neurologist who recognizes visual snow syndrome.
- Explore supportive interventions: tinted lenses, screen adjustments, and sleep improvements are low-risk first steps.
- Connect with others: peer communities offer validation and practical tips, but be mindful of unverified medical claims.
- Prioritize mental health: persistent sensory disturbance can be stressful; cognitive behavioral strategies and counseling can help coping.
CONCLUSION — WHAT THE RISE IN AWARENESS TEACHES US
The story of visual snow's rise from obscurity to recognized syndrome is about more than one condition. It illustrates how lived experience, patient communities, and clinician curiosity can transform medical knowledge. When people stop assuming their experience is unique and start speaking collectively, patterns emerge, research follows, and medicine changes. For individuals, that change can mean validation, better diagnostic pathways, and the hope—however tentative—of targeted treatments. For medicine, it is a reminder that listening matters: symptoms that once seemed rare often sit at the edge of discovery, waiting for a language to bring them into view.
There remains work to do: better prevalence estimates, more effective treatments, and deeper mechanistic understanding. But one immediate truth has been established: visual snow stopped being rare not because it suddenly appeared, but because people finally found the words and networks to say, together, 'this is what I see.' That shared sentence created a new medical reality—one in which the static is no longer just noise, but a call to understand the human brain and its fragile, remarkable way of creating the world we see.