
The Line on My Pinky Nail: A Subungual Melanoma Story
I first noticed it in a photograph: a thin, cigarette‑paper line running from base to tip along the pinky nail of my left hand. At the time it was 1–2 millimeters across, steady and quiet, like a faint pencil mark under a translucent roof. For eight years it lived in the margins of my life — something to ignore when typing, something to blame on a manicure, something my busy brain told me was harmless. It took a routine skin check, a dermatologist who asked the right questions, and a biopsy I had put off for too long to learn it was not a cosmetic quirk but a rare form of skin cancer: subungual melanoma.

longitudinal melanonychia
How a Small Line Became a Long Story
The story is painfully ordinary. A tiny change, a long delay, a cascade of explanations that sounded plausible: pigment from a splinter years before, a fungal stain, a harmless matrix nevus. People said I should stop worrying. I stopped photographing my hands and learned to look away when strangers asked what happened to my nail. The line didn’t hurt. It didn’t itch. It simply existed, and that made it invisible — until someone trained to notice nail pigment asked whether it had widened or darkened at the proximal cuticle.
The truth about nail pigment is that small differences matter. Dermatologists use a vocabulary I hadn’t known — longitudinal melanonychia for a lengthwise stripe, Hutchinson sign for pigment extending onto the surrounding skin, pseudohutchinson when pigment shows only through the cuticle — and they listen for change. For me, the difference between “a line” and “a symptom” was a matter of inches and months: the band had grown slightly and its edges looked ragged when examined with a dermatoscope. Those details, in the hands of an experienced clinician, led to a biopsy.

nail cancer dermatoscope
What Those Lines Are: Medical Explanation
Longitudinal melanonychia describes a brown or black stripe that runs from the proximal nail fold toward the free edge. It can come from benign sources — ethnic pigmentation, nevi (moles) in the nail matrix, trauma, or medications — or from malignant ones, most notably subungual melanoma. Nail unit melanoma arises from melanocytes within the nail matrix and is most commonly an acral lentiginous subtype. It is uncommon but consequential: because it develops where detection is more difficult, diagnosis is frequently delayed.
Clinicians watch for several red flags when assessing a pigmented nail band:
- Width: Bands wider than roughly 3 mm deserve closer scrutiny.
- Color and evolution: Darkening, variegated pigment (different shades), or new-onset pigment in adulthood.
- Border irregularity: Uneven, blurred, or jagged lateral edges rather than a uniform stripe.
- Proximal widening: A band that broadens near the cuticle.
- Hutchinson sign: Pigment extending onto the proximal or lateral nail folds (not to be confused with pseudo‑Hutchinson).
- Associated nail dystrophy: Splitting, bleeding, ulceration, or nail plate destruction.
None of these alone confirms cancer, but together they raise clinical suspicion. For my case, the combination of gradual width increase, uneven borders, and a subtle micro‑Hutchinson sign seen under dermoscopy changed the conversation from watchful waiting to tissue sampling.

Hutchinson sign nail
The Diagnostic Path: Biopsy Types and What They Tell You
Biopsy of the nail unit is a technical challenge. The nail matrix — the tissue that produces the nail plate — lies beneath delicate structures, and sampling it risks permanent nail changes. Dermatologic surgeons choose the approach that balances diagnostic accuracy with cosmetic outcome:

subungual melanoma biopsy
- Punch biopsy: Useful for narrow bands originating in the distal matrix. It is quick but can miss peripheral disease if the band is wide.
- Lateral longitudinal excision: Removes a full‑thickness strip of the nail apparatus; favored for suspicious lateral lesions because it samples matrix, bed, and hyponychium.
- Tangential (shave) excision: Less invasive and associated with minimal dystrophy; sometimes used for mid‑plate lesions with intermediate suspicion.
- Full‑thickness matrix biopsy: The gold standard when invasive melanoma is suspected; it gives the pathologist the depth measurement (Breslow thickness) needed for staging.
My dermatologist recommended a tangential excision at first because the lesion’s appearance was borderline; she warned that if the pathologist saw anything concerning, I would need a full‑thickness sampling. The day of the procedure I felt a strange mix of relief and dread: relief that someone was finally looking, dread about the possibility of missing work, and the very real fear that my life might change.
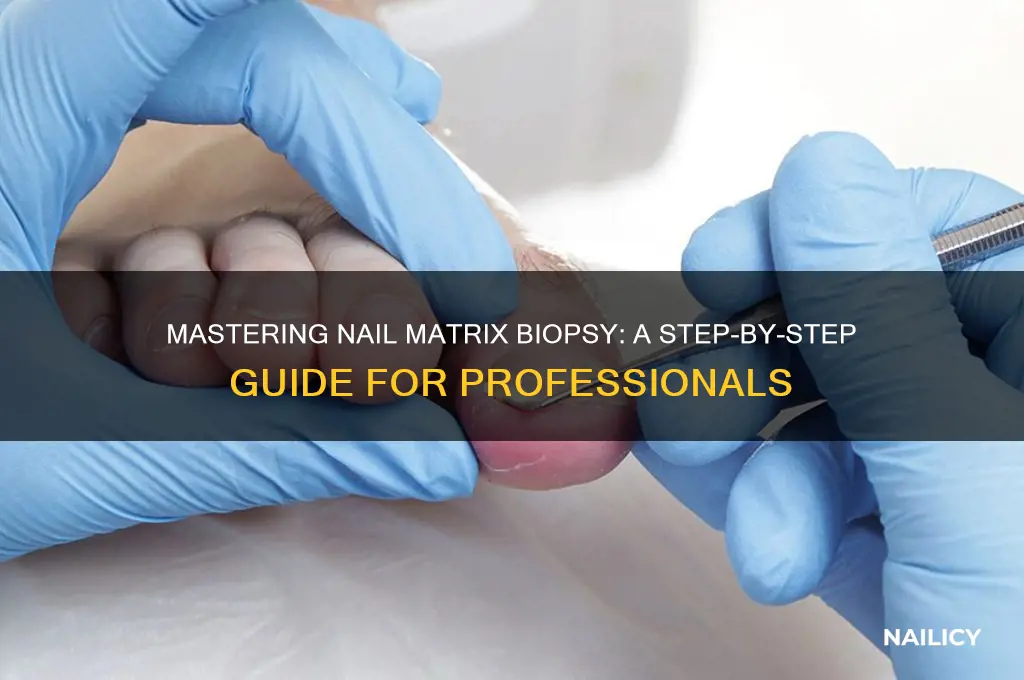
nail matrix biopsy
When the pathology report used the word melanoma, the shock arrived in a clinical sentence. I learned later about staging, about Breslow depth as the best single predictor of outcome, and about how subungual melanoma—because of its location—sometimes presents with a superficially lentiginous growth that can mask deeper invasion. I also learned that whether a melanoma is pigmented or amelanotic (lacking dark pigment) matters for recognition but not for seriousness.

pinky nail melanoma
Why These Tumors Are Rarely Detected Early
Subungual melanoma is uncommon in many populations, which is part of the problem. It accounts for a small percentage of all melanomas in light‑skinned groups, and a higher proportion in individuals with darker skin types. The reasons for delayed detection include:
- Location — people rarely inspect nails closely, and clinicians may overlook the nail as part of routine skin checks.
- Misdiagnosis — pigment can be blamed on hematoma (subungual blood), fungal infection, or trauma.
- Variation in presentation — some nail melanomas are amelanotic or present with nail destruction rather than pigment.
Many patients describe teachers, barbers, or spouses noticing the change before they did. Others are told, repeatedly, that it is nothing. That inertia costs time. In my case, the lesion’s slow, quiet change allowed the disease to grow inches under my attention and habit.
"The band had grown slightly and its edges looked ragged when examined with a dermatoscope — those small details changed everything."
Treatment Options and What to Expect
Treatment is individualized. For in situ or very thin lesions, conservative wide local excision of the involved nail unit with reconstruction may be curative. For invasive tumors, treatment can include wider excision, partial removal of the distal phalanx, or—less commonly now—more proximal amputation of the finger or toe. Decisions are influenced by Breslow depth, ulceration, and whether there is spread to regional lymph nodes.
Sentinel lymph node biopsy is considered when the primary tumor reaches thresholds that suggest risk of occult nodal disease. Nodal involvement changes staging and often prompts systemic therapy discussions. In recent years, advances in targeted therapies and immunotherapy have transformed outcomes for many melanoma patients, particularly those with advanced disease. The emotional tenor of treatments also varies: living with the visible effect of nail surgery can be a profound adjustment, and many patients value reconstructive approaches when appropriate.
Emotional and Practical Realities
Beyond clinical terms, cancer imposes practical burdens: time off work, repeated clinic visits, insurance paperwork, and the slow recalibration of identity when an ordinary body part becomes tied to risk. For months I cataloged every hand movement as if it might reveal residual disease. I learned to ask different questions at appointments: What is the stage? What are the margins? When will the next imaging or dermatology visit be? I learned to bring a trusted friend to difficult conversations.
A Practical Checklist: When to See a Doctor
If any of the following apply, arrange an evaluation with a dermatologist rather than waiting:
- New single‑nail pigment in adulthood that is not clearly due to trauma.
- Band wider than 3 mm or a band that is increasing in width.
- Irregular borders, variegated color, or proximal widening.
- Hutchinson sign — pigment on adjacent skin or cuticle.
- Nail dystrophy such as splitting, bleeding, or lifting (onycholysis).
- Any rapid change in color or shape of a pigmented band.
Lessons from an Eight‑Year Wait
The hardest lesson was that waiting can feel like strength when it is really avoidance. My delay had reasons: life was busy, providers had reassured me, and the lesion was small. But the biology of melanoma does not negotiate with reassurance. Early detection matters. So does clear communication with clinicians: ask them to explain the degree of suspicion in concrete terms, what monitoring would look like, and at what point a biopsy would be recommended.
- Single, changing pigmented bands on a nail deserve evaluation by a dermatologist.
- Red flags include width >3 mm, irregular borders, Hutchinson sign, and nail dystrophy.
- Biopsy is the definitive test; techniques vary to balance accuracy with cosmetic outcome.
- Subungual melanoma is rare but can be serious; earlier detection improves treatment options.
Closing Thoughts
I could rewrite the eight years as a parable about vigilance, but the better truth is practical: our bodies whisper before they shout. Small, odd changes sometimes signal nothing. Sometimes they signal everything. If you have a single, new, or changing pigmented streak on a nail, it is worth the few hours it takes to get it evaluated. For me, that visit changed a line into an answer and an anxiety into a plan. The scar on my pinky is a reminder — not only of what happened, but of what I learned: to look, to listen, and to act when the body asks for attention.
If you notice a new or changing line on a fingernail or toenail, make an appointment with a dermatologist; timely evaluation can change outcomes.