
Syringe Reuse in Pakistan Hospital Infects 331 Children with HIV

Larkana Pakistan clinic
The headline is stark and the human cost immediate: 331 children tested HIV-positive after being given injections at a single medical facility where syringes were reused. For families, what began as routine care—vaccinations, intravenous fluids, or injections for fever—turned into a life-altering medical crisis. For public health officials, the incident became a glaring alarm about gaps in oversight, infection control, and the fragile bridge between informal healthcare delivery and safe modern medicine.

Pakistan hospital injection
BACKGROUND: What Happened and Why It Matters
A local practice with global implications
Unsafe injection practices are a long-recognized driver of bloodborne disease transmission. In many low- and middle-income settings, injections are common, often preferred by patients and providers alike for their perceived immediacy of effect. But when single-use items are reused or sterilization is incomplete, the risk of transferring viruses such as HIV, hepatitis B and hepatitis C becomes real and measurable. An outbreak in which hundreds of children are infected in a short span forces us to confront how easily trust can be broken and preventable diseases can spread through routine care.
Immediate public health consequences
Beyond the horror of each family's diagnosis, such an outbreak creates multiple cascading problems: a sudden demand for pediatric HIV testing and antiretroviral therapy (ART), the need to trace potentially exposed contacts, and the urgency of halting ongoing unsafe practices at the facility and beyond. The emotional and economic toll is enormous: caregivers face stigma and financial strain while health systems scramble to deliver lifelong treatment and psychosocial support.
"This was routine care that became a vector for a chronic disease—preventable, if standard infection control had been followed."

syringe needle reuse
HOW IT HAPPENED: Mechanics of Transmission
The fatal step: reusing syringes and needles
HIV is transmitted when blood or blood-containing fluids from an infected person enter another person's bloodstream. A syringe or needle carrying even microscopic amounts of infected blood can introduce virus directly into tissue or a vein. In practice, transmission risks are highest with shared needles among people who inject drugs, but any clinical reuse of injection equipment without validated sterilization can have the same effect.
Factors that enable reuse
Several systemic drivers commonly contribute to reuse: limited supply chains for disposables, cost-cutting at small or unregulated clinics, lack of staff training, and inadequate regulatory enforcement. Patients may also request injections because they associate them with stronger cures, creating a demand-side pressure on providers. When a clinic operates with informal finances and weak oversight, the incentives to cut corners multiply.
THE HUMAN TOLL: Children, Families, and Communities
Beyond numbers: stories behind the statistic
Every one of the 331 children is a person with a family, a routine, and a future upended. Parents describe routine visits for fever, diarrhea, or dehydration—common childhood illnesses—and a trust that the doctor’s office is safer than the playground. That trust is now fractured. Families face medical appointments for baseline HIV staging, immediate linkage to pediatric ART, and long-term monitoring, while navigating the psychological consequences and community stigma that often follows public disclosure of HIV cases.
Parents said they trusted injections because clinicians there promised fast relief; instead their children received a lifetime diagnosis.Stigma and social fallout
Social stigma around HIV remains powerful in many societies. Families may avoid testing or care because they fear ostracism, and children can face exclusion at school or in social settings. Public health responses must therefore include confidentiality protections, counseling, and community education to prevent blame and to encourage treatment adherence.
pediatric HIV testing
MEDICAL RESPONSE: Testing, Treatment, and Follow-Up
Testing scale-up and contact tracing
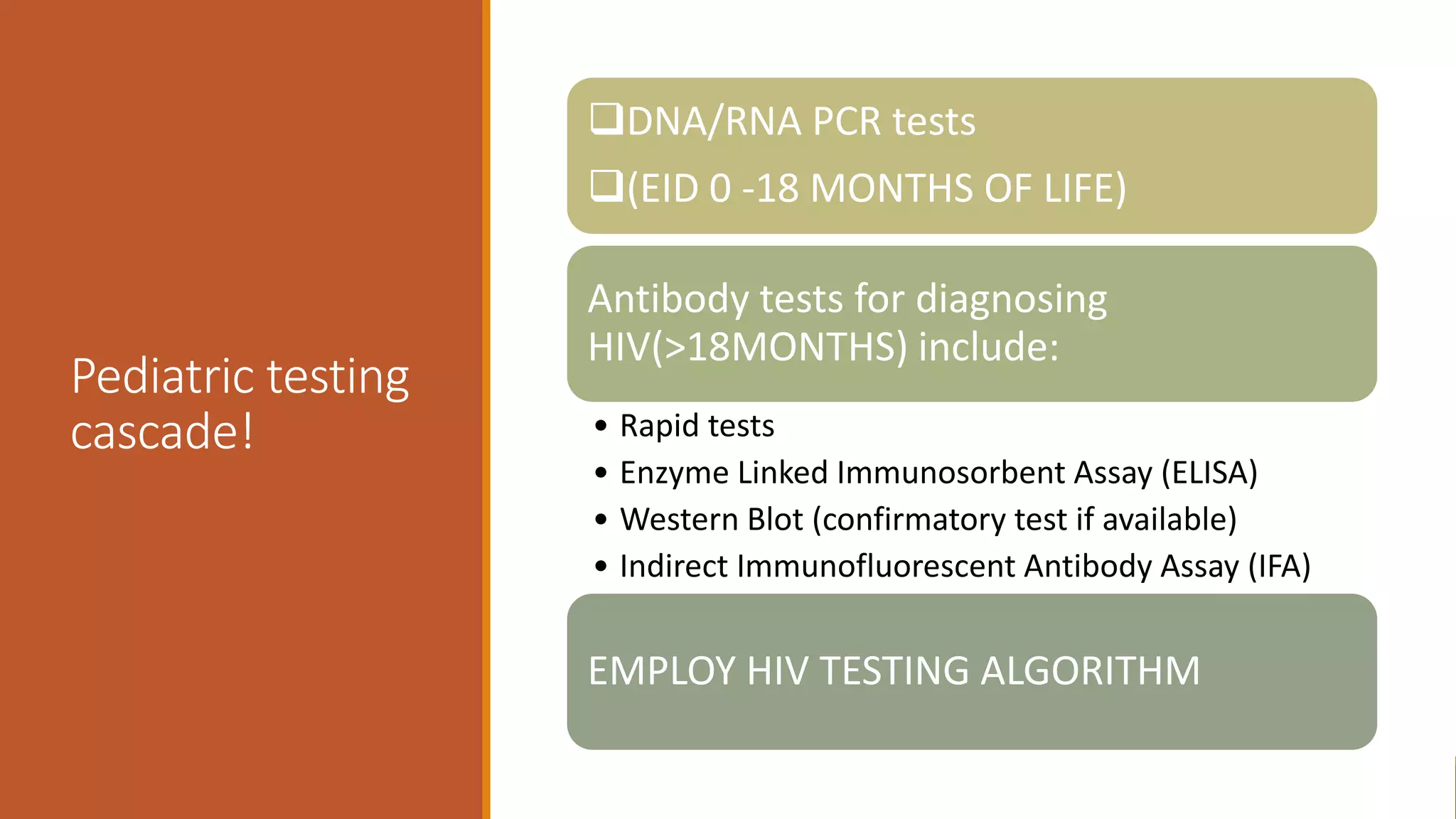
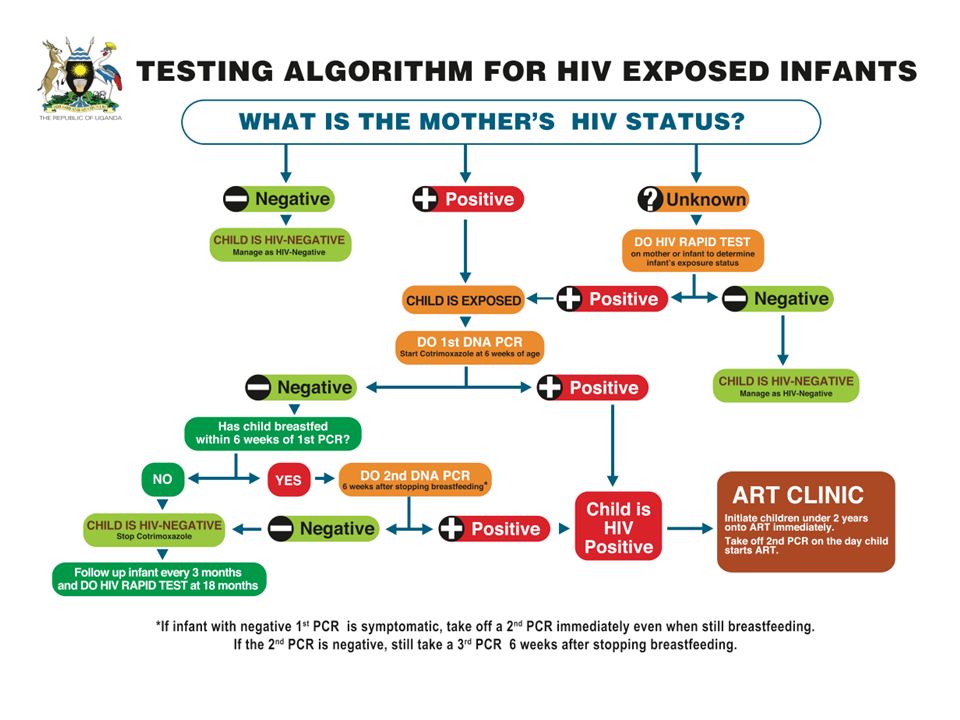
A central part of outbreak control is rapidly identifying who was exposed. That means mass testing of children who visited the facility during the risk window, screening family members, and employing contact tracing to find others who may have been injected there. For children, antibody testing can be complicated by maternal antibodies in infants under 18 months; specialized nucleic acid tests may be required to confirm infection in very young children.
Linkage to pediatric ART
Once diagnosed, immediate linkage to pediatric antiretroviral therapy is lifesaving. Modern ART dramatically reduces morbidity and mortality and suppresses viral load to undetectable levels, improving quality of life and preventing onward transmission. Challenges in this setting include securing pediatric formulations, ensuring supply chain continuity, dosing adjustments for weight and growth, and long-term adherence support for caregivers.
children HIV treatment
SYSTEM FAILURES: Regulation, Oversight, and Accountability
Where the system broke down
Outbreaks of this nature rarely stem from a single reckless act. They are typically the result of multiple system failures: weak regulatory inspections, under-resourced public clinics pushing patients to private providers, and fragmented medical supply chains that leave some clinics chronically short of disposables. In many countries, a parallel economy of small clinics operates outside formal oversight—licensed, semi-licensed, or entirely informal—where training and accountability are inconsistent.
Legal and ethical considerations
Public anger often demands legal accountability, and rightly so. Prosecutions, licensing suspensions, and fines can play a role in deterrence. But courts and regulators must also balance criminal blame with the need to strengthen systemic capacity: retraining staff, improving supply logistics, and rebuilding trust through transparent remediation. Ethical response includes compensation schemes, long-term care commitments, and careful communication to avoid retraumatizing families.
"Accountability is not only punishment; it is a promise to rebuild safer systems for the next child who enters a clinic."
PREVENTION: Practical Steps to Stop Syringe Reuse
Supply-side interventions
Ensuring an uninterrupted supply of single-use syringes and needles is foundational. Procurement contracts, bulk purchasing, and logistics management must prioritize consistent delivery to clinics. Where supply chains are unreliable, low-cost safety-engineered syringes that prevent reuse can be lifesaving. Proper disposal systems, including puncture-proof sharps containers and regulated waste collection, reduce incentives to salvage and reuse equipment.
Training and behavior change
Clinician behavior is influenced by training, supervision, and norms. Regular in-service training in injection safety, checklists for procedures, and supervisory audits help normalize best practices. On the demand side, community education that explains the risks of unnecessary injections and promotes oral alternatives for many conditions can reduce pressure on providers to prescribe injections as a default.
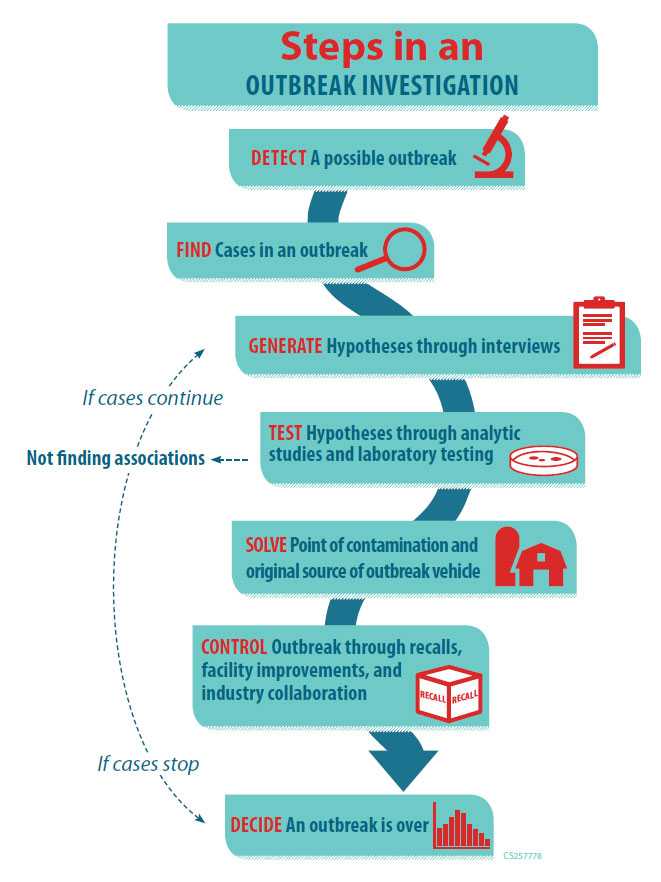
public health outbreak investigation
COMMUNITY RESPONSE: Trust, Communication, and Support
Engaging caregivers and local leaders
Transparent, empathetic communication is essential. Public health teams must explain what happened, what is being done, and what families can expect in terms of testing and treatment. Partnering with community leaders, religious figures, and school authorities helps reduce stigma and restore trust. Mental health services and peer support groups for affected families can mitigate trauma and isolation.
Maintaining confidentiality
Because stigma can drive families away from care, confidentiality safeguards must be rigorously enforced. Mobile testing sites, anonymized appointment systems, and private counseling can help ensure that children are brought into care without fear of public exposure.
WIDER LESSONS: What This Outbreak Tells Us About Global Health
Prevention is far cheaper than treatment
From a cost perspective, preventing transmission through basic injection safety measures is orders of magnitude cheaper than the lifelong cost of treating pediatric HIV. Investments in procurement, training, surveillance, and robust regulatory systems yield outsized returns in both health and economic terms.
Equity and access
Outbreaks like this often occur where health systems are stretched thin. Strengthening primary care, improving supply equity, and formalizing informal providers are long-term strategies that reduce reliance on risky practices. International partners can provide technical support, but sustainable change depends on domestic commitment and resources.
- Clear pathway to prevention through disposable supplies and training
- Rapid testing and ART can reduce long-term harm
- Existing stigma complicates case finding and care
- Resource gaps make systemic fixes slow
WHAT PARENTS AND CLINICIANS NEED TO KNOW
For parents
If your child received an injection at the affected facility, get them tested and linked to care immediately. Early diagnosis and treatment dramatically improve outcomes. Ask the clinic for a written record of visits and request clear instructions for follow-up care. Seek counseling to manage the emotional impact and connect with other families for peer support.
For clinicians and facility managers
Review supply inventories and disposal practices today. Conduct rapid staff retraining on injection safety, implement a no-reuse policy with visible enforcement, and report any lapses through official channels. Engage with public health authorities to support contact tracing and prioritize patient communication.
"Immediate, compassionate action and long-term system repair are both required—one without the other leaves families exposed."
CONCLUSION: Repairing Trust, Preventing Future Harm
This outbreak is both a tragedy and a clarifying moment. It shows how preventable mistakes can spiral into chronic illness for children and long-term burden for families and health systems. The path forward is practical: ensure reliable supplies of disposables, strengthen regulation and training, expand testing and treatment access, and rebuild trust through transparent, empathetic communication. Accountability matters, but so does an investment in systems that make reuse impossible.
- 331 children were diagnosed after syringe reuse at a single facility, highlighting a grave failure in infection control.
- Prevention through supplies, waste disposal, and training is far more cost-effective than treating chronic infections.
- Rapid testing, immediate linkage to pediatric ART, and protection from stigma are central to the medical response.
- Systemic reform—procurement, regulation, and community engagement—must follow to prevent recurrence.
Final thought
Healthcare is a contract of trust. When basic safety measures fail, the wound extends beyond biology into the social fabric of a community. The urgent work is twofold: care for the children already harmed, and change the systems that allowed harm to happen in the first place.