
Syringe Reuse in Pakistan Hospital Infects 331 Children
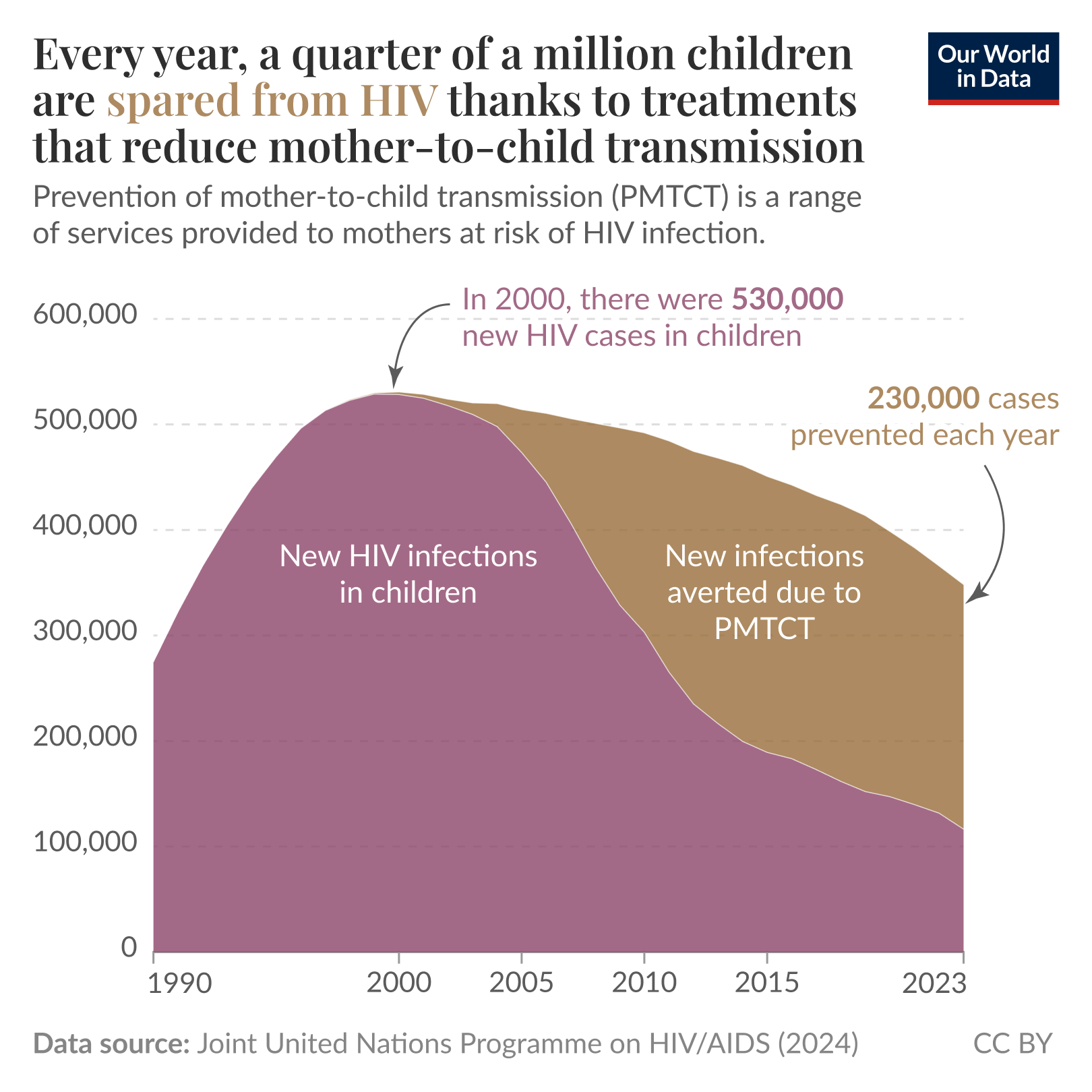
The headline is blunt and horrifying: 331 children infected with HIV after syringes were reused at a hospital in Pakistan. Behind that stark number are families shattered by a preventable infection, clinicians who work in pressured conditions, and a health system whose gaps made transmission possible. This article reconstructs how syringe reuse leads to outbreaks, explores the systemic drivers that allow it to occur, and lays out what can be done at the bedside, in clinics, and at policy level to ensure the same mistake is not repeated.

Pakistan hospital injection safety
What Happened — The Anatomy of an Outbreak
The immediate chain
At its simplest, the episode began with repeated needle and syringe use in settings where single-use devices should be discarded. A child receives an injection, the device is not disposed of properly, and that same needle or syringe is used on another patient. If the first child carried bloodborne pathogens — for example HIV — the contaminated device can transfer infectious material to the next patient. Repeat that process dozens or hundreds of times and the number of new infections grows quickly.
children HIV infection outbreak
Why children are uniquely affected
Children are often brought repeatedly to clinics for routine care: vaccinations, fever, dehydration, or local injections for minor ailments. In settings where injections are common and disposable supplies are scarce, children can be disproportionately exposed. Their caregivers, relying on advice from trusted clinicians, rarely have the power or knowledge to insist on single-use practices.
A preventable lapse in routine technique became the vector for tragedy — and revealed layers of systemic weakness.

pediatric hospital care Pakistan
Why Syringe Reuse Happens
Supply and logistics
At the most basic level, syringe reuse often reflects supply-chain problems: inconsistent deliveries of single-use syringes, budget constraints, and lack of accessible disposal containers. When a clinic runs out of disposables, the temptation to reuse is immediate. In underfunded settings, procurement cycles can leave gaps, and buying large stocks may be impossible for smaller facilities.

medical supply chain Pakistan
Training and culture
Clinical habits are formed by training and reinforced by workplace culture. If staff have never seen strict injection safety enforced, if senior clinicians model reuse or improvisation, junior staff will normalize those behaviors. Time pressure, heavy caseloads, and informal payments for injections can further distort safe practice.
How HIV Travels Through a Needle
The biology
HIV is present in blood and certain body fluids. A needle or syringe that draws blood from an infected person may retain microscopic blood residues. If that device is used again without effective sterilization, those residues can be injected into another person's bloodstream. The risk depends on the amount of blood, the virus concentration, and the interval between uses, but any reuse of injection equipment carries risk for bloodborne infection.
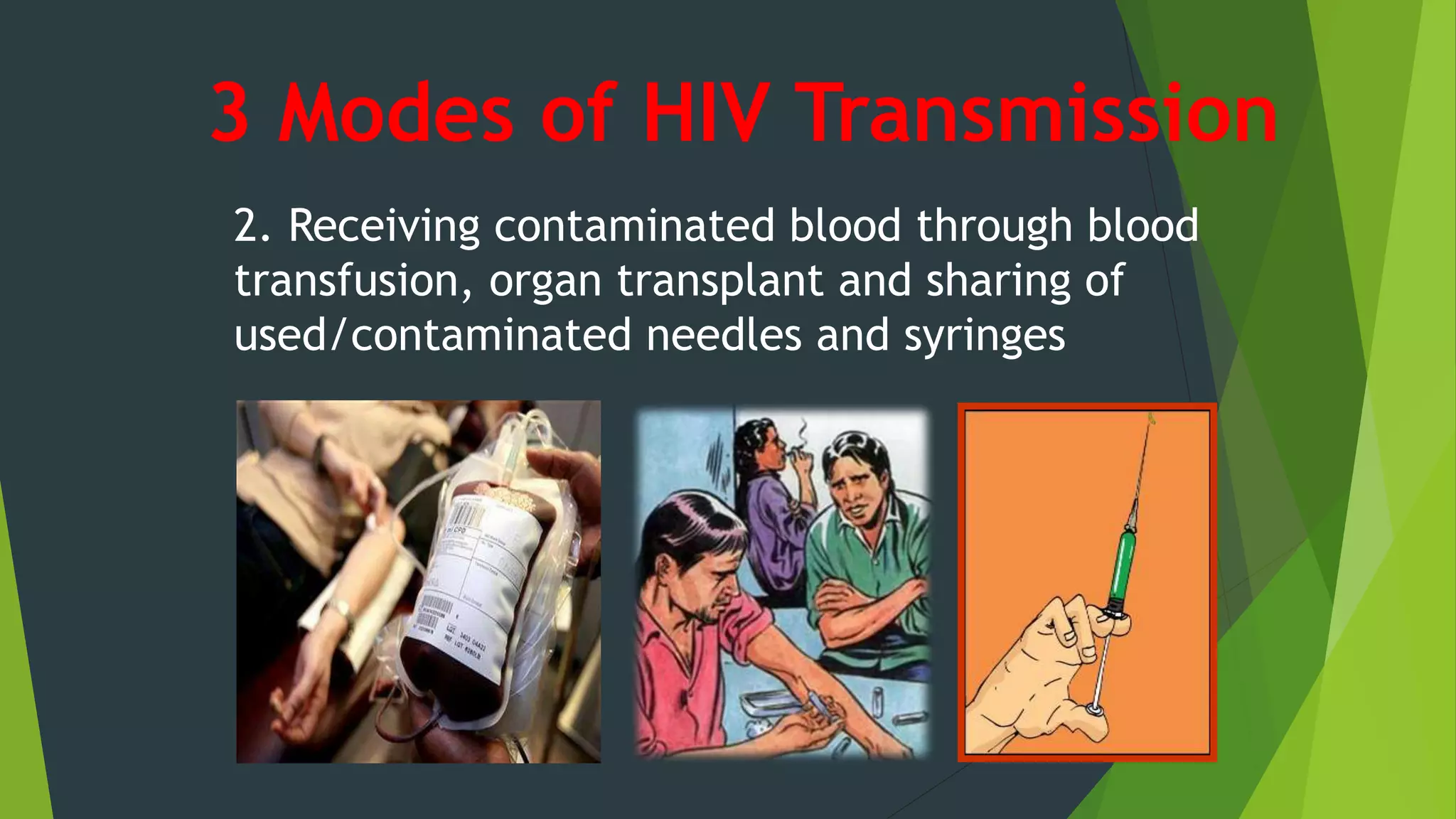
HIV transmission contaminated needles
Why makeshift sterilization fails
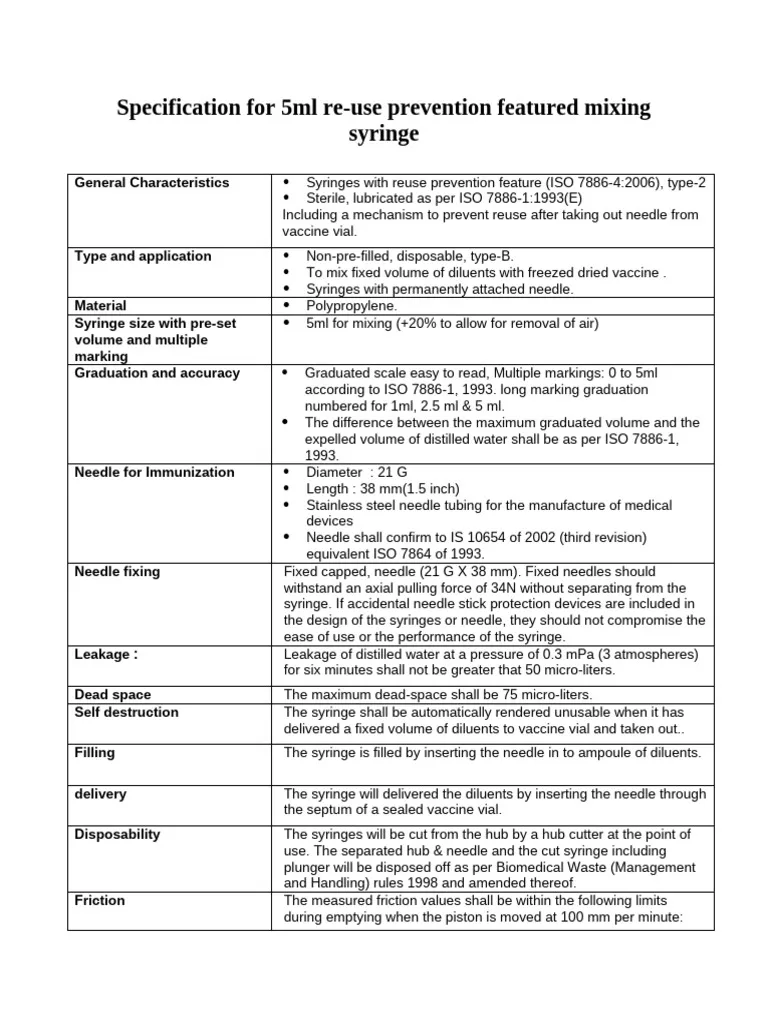
In some settings, staff attempt to sterilize and reuse equipment using boiling or chemical rinses. These methods are unreliable for needles and syringes because internal surfaces and small lumens can trap blood. Autoclaves and validated sterilization protocols work for many tools — but not for disposable syringes meant for one-time use.
Systemic Failures That Amplify Risk
Weak regulation and oversight
Regulatory systems that fail to monitor injection practices create blind spots. Routine audits, licensing checks, and spot inspections can deter unsafe behavior. Where oversight is fragmented or under-resourced, risky shortcuts become more likely and less visible.
syringe reuse contamination prevention
Economic incentives and informal practices
In many places, injections are perceived by patients as more effective than oral medication. That demand, combined with providers' ability to earn informal fees for administering injections, creates an incentive to give injections even when they aren't medically necessary. Overuse multiplies opportunities for error and reuse.

single-use syringes medical supplies
Human Toll and Community Impact
Families and stigma
When children test positive for HIV in such an outbreak, families face medical, emotional, and social upheaval. Caregivers may blame themselves; communities may stigmatize affected children; schooling and social participation can be disrupted. Public trust in the health system erodes, and parents may avoid care or vaccination in fear of further harm — a dangerous secondary effect.
Long-term care needs
Children infected with HIV require lifelong follow-up: antiretroviral therapy, monitoring, and psychosocial support. That commitment falls on families and health systems already stretched by limited resources, creating a chronic burden from a single preventable lapse.
Investigation and Response: What Authorities Must Do
Immediate steps
Following detection of clustered infections, rapid response teams should: test exposed contacts, provide post-test counseling, begin antiretroviral therapy for those infected, and halt unsafe practices through clear directives. Transparent communication with affected families and the public is vital to maintain trust and to ensure people seek testing.
Forensic epidemiology
Outbreak investigators use case histories, timelines, and laboratory data to reconstruct transmission chains. Identifying whether infections are linked to a single source or multiple sources (for example, blood transfusions versus injections) guides both immediate containment and long-term policy changes.
Prevention: Practical, Scalable Measures
Ensure supply and safe disposal
Guaranteeing consistent availability of single-use syringes and appropriate sharps containers is the foundational step. Procurement plans should include buffer stock and rapid resupply mechanisms for high-use facilities. Proper sharps disposal prevents scavenging and reuse outside the clinic.
Strengthen training and workplace norms
Regular, competency-based training that includes practical demonstrations, supervision, and corrective feedback reduces unsafe habits. Facilities should create visible standards — for example, a single-use policy poster — and enforce them through routine observation and accountability measures.
Policy and incentive alignment
Policies that remove perverse incentives (for example, banning informal fees for injections) and that reimburse evidence-based care discourage unnecessary injections. Regulation should be paired with support so clinics can comply without jeopardizing operations.
What Families and Communities Can Do
Ask questions, demand transparency
Patients and caregivers have the right to know if syringes are new and single-use. Asking to see the needle and the sealed package before an injection is a reasonable request. Community education campaigns can normalize these questions and reduce the power imbalance between providers and families.
Seek testing and support
Anyone who fears exposure should seek testing and counseling promptly. Early diagnosis improves outcomes, and antiretroviral therapy can control the virus and prevent further transmission. Importantly, communities must support affected families and protect children from discrimination.
Broader Lessons for Global Health
Low-tech failures, high-impact consequences
This outbreak is a reminder that modern medicine's greatest vulnerabilities are sometimes not exotic pathogens but simple lapses in routine safety. A single-use device exists for a reason; when systems fail to uphold basic standards, the consequences ripple outward.
The role of donors and international agencies
International partners can support supply chains, training programs, and surveillance capacity. But sustainable change demands domestic ownership: national policies, effective regulatory systems, and political will to fund and enforce safe practices.
Prevention of bloodborne outbreaks is cheap relative to the lifetime cost of care — but it requires attention to detail, not headlines.
Conclusion
The infection of hundreds of children following syringe reuse is a wrenching example of how avoidable lapses in basic infection control can create long-term suffering. The path to prevention is clear: secure supplies, enforce single-use policies, invest in training and supervision, and empower communities to expect safe care. When systems and people align around those simple practices, we protect the most vulnerable: children, whose futures depend on adult decisions made today.
- Syringe reuse is preventable: ensure uninterrupted access to single-use devices and sharps disposal.
- Training and culture matter: supervision, accountability, and norms reduce risky behavior.
- Families must be empowered: informed patients can demand safe practice.
- Policy and oversight are essential: regulation paired with support reduces systemic risk.
This article examines systemic causes and prevention strategies following a major needle- and syringe-related outbreak affecting children in Pakistan.