
Surviving Brain Cancer and Diabetes Insipidus: My Halloween Finish
The year I was diagnosed—2008—feels like a decade of days and a lifetime compressed into one calendar. I remember the sterile hush of the clinic, the way fluorescent lights could make a person feel transparent, and the moment a doctor first said the words that would change everything: "brain tumor" and "a condition causing extreme urination." The numbers he used were hard to imagine—liters where I had only ever thought in cups. Later, someone would clock my daily output at roughly 11 gallons. To put it plainly, my body had rewritten its plumbing overnight.
11 gallon urine output daily
"When I learned that I was producing roughly 11 gallons of urine a day, the practicalities of survival—where to sleep, how to leave the house, which clothes to wear—became as urgent as any medical decision."
THE DIAGNOSIS
The first diagnosis felt like a foreign language. Tests blurred into one another—MRI scans, blood panels, fluid balance charts—and each result created a new landscape of questions. What kind of tumor? Where exactly was it? Could it be removed? Then there was the other, stranger problem: my thirst was unquenchable, and my body reacted to drinking by producing what felt like unstoppable rivers.
Understanding the immediate clinical picture
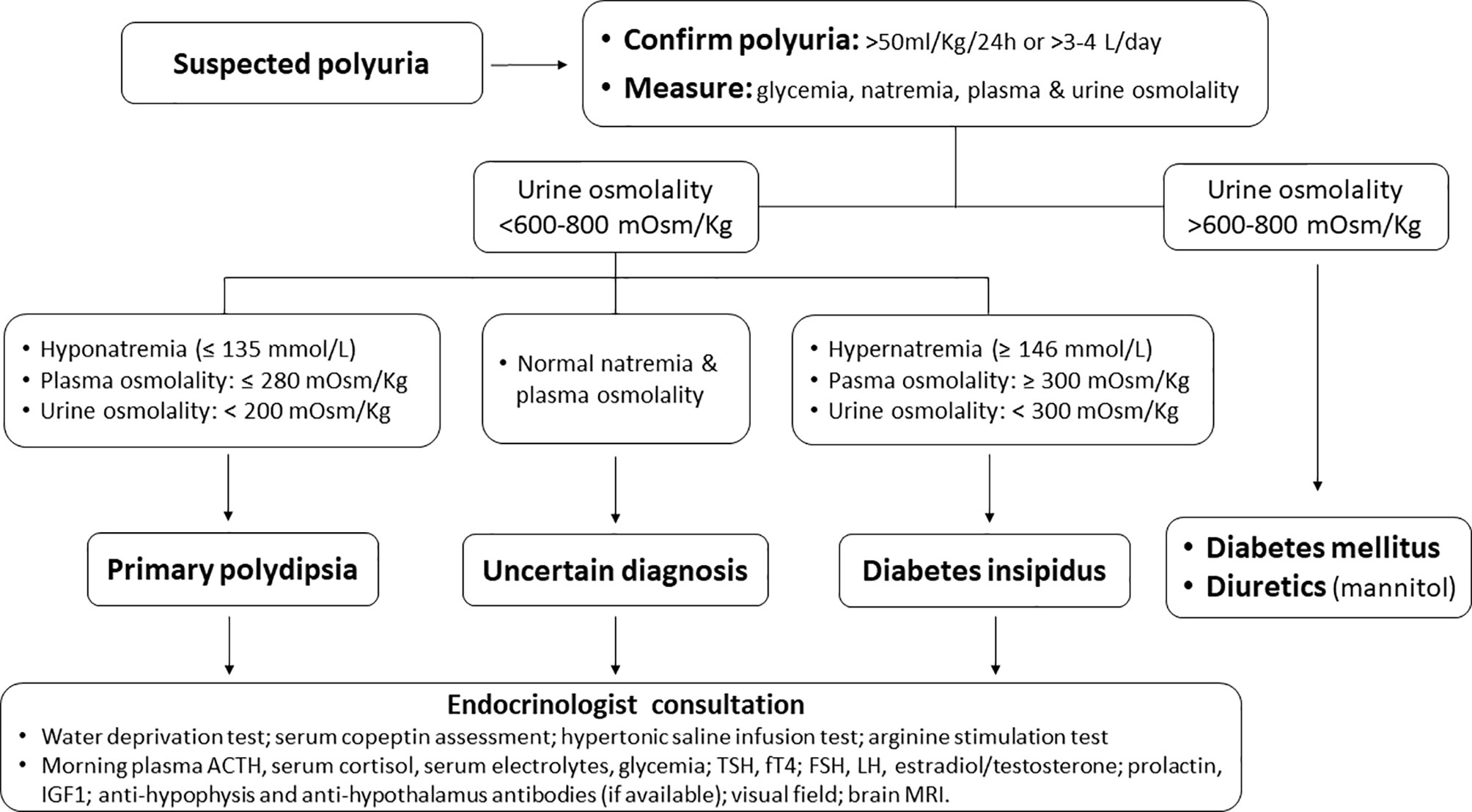
My case combined two medical realities. The brain tumor itself demanded attention, but the symptom that dominated daily life was extreme polyuria: the medical term for producing abnormally large volumes of urine. In my case, that translated to volumes most clinicians see only in textbooks or the occasional dramatic case report. The endocrinology team suspected diabetes insipidus (DI), a disorder where the kidneys cannot concentrate urine because of a deficiency or resistance to antidiuretic hormone.
central diabetes insipidus diagnosis
Conversion so the number sinks in
Numbers can anesthetize or they can orient. Eleven gallons equals about 41.6 liters. Imagine carrying home a case of 40 one-liter bottles every single day and having to empty them again and again. That is the kind of logistics my life required for a while.
UNDERSTANDING THE CONDITION
There are two main types of diabetes insipidus relevant to someone with a brain tumor: central DI and nephrogenic DI. Central DI arises when the brain's production or release of antidiuretic hormone (also called vasopressin) is disrupted—often because of injury to the hypothalamus or pituitary gland. Nephrogenic DI happens when the kidneys don't respond to vasopressin. In my situation, the tumor and subsequent treatments had interfered with normal pituitary function, and the endocrinology team treated me as if I had central DI.
Why this matters clinically
When the body loses that much water daily, multiple systems go out of balance. Electrolytes—particularly sodium—can swing to dangerous levels. Dehydration risks increase even when a person is drinking constantly because fluid leaves faster than it can be retained. The goals of treatment are pragmatic: prevent dangerous sodium shifts, keep the patient hydrated, and address the underlying cause if possible.
LIVING WITH 11 GALLONS A DAY
Most medical narratives focus on imaging, surgeries, and medication names. That's important. But there is a parallel story about how illness rewires the ordinary logistics of life. My days became a choreography of bathrooms and bottles. Leaving the house meant calculating timings, knowing where restrooms were, and dressing for rapid, discreet access. Sleep was punctuated by trips to the bathroom and the constant anxiety of what would happen if a catheter or collection device failed.
Practical adaptations
- Clothing: I switched to loose trousers and clothing with easy closures so I could move quickly without drawing attention.
- Scheduling: I planned appointments and outings around places with reliable bathrooms, and I learned to map my city by restroom availability.
- Hydration tools: I carried multiple insulated water containers and a small cooler during long days to keep fluids cold and palatable.
- Privacy strategies: I developed soft scripts to explain sudden bathroom needs to colleagues and friends without having to divulge medical details I wasn't ready to say aloud.
All of this required a level of vigilance and, ironically, a sense of humor. When you live with an absurd daily volume of urine output, it helps to be able to laugh at the absurdity sometimes.
TREATMENT AND RECOVERY
Treating central DI often involves replacing or mimicking the antidiuretic hormone. For many people, desmopressin (known by brand names such as DDAVP) becomes a cornerstone of care. The dose, formulation, and route—oral, nasal, or injectable—are individualized because the balance between under-treatment and over-treatment can be dangerous.

desmopressin medication for diabetes insipidus
Medical milestones
My recovery had clear milestones: stabilize sodium, find a workable dose of medication, reduce night-time disruptions, and—when possible—address the tumor that had started this cascade. Radiation and surgery were part of that path, but it was the endocrinology clinic that helped me reclaim the day-to-day. With careful titration, my urine volumes decreased. The terrifying daily calculations eased. Most importantly, the fear that my body would continue to drain itself unchecked began to recede.

pituitary tumor treatment
The slow work of rebuilding stamina
Recovery from cancer and from a complication like DI is not linear. Energy returned in increments. Some days I felt normal; others were reminders of fragility. Physical therapy and gentle exercise helped rebuild cardiovascular stamina that had eroded during intensive treatment. Mental health care—psychotherapy and support groups—helped me process fear, grief, and survivor guilt.
"Treatment changed my body, but community and small rituals helped me find a life again."
THE HALLOWEEN COSTUME
When I finally reached a milestone—when my oncologist said 'finished' and my endocrinologist agreed that we had a manageable regimen—it felt like a rebirth. I wanted the world to know I had survived, but I also wanted to carry the story of what I had lived through with a wink instead of a sob. Halloween that year became the stage.
Designing the costume
Friends and I talked about something clever, not grim. We wanted a costume that acknowledged the absurd volume of my urine output without fetishizing the illness. The idea landed on an oversized, 11-gallon 'hydration pack'—a transparent wearable bag filled with empty labeled bottles, a big cardboard tag that read "Survivor: Hydrated and Here", and a small, comical stethoscope pinned like a medal. I wore ankle boots and a coat with easy access pockets; people thought I was a walking water cooler, and most laughed immediately. Children asked, adults smiled, and a few nurses from my old clinic recognized me and hugged me for reasons beyond words.
hydration pack costume for Halloween
Caption: The costume was equal parts defiance and rejoicing—funny, human, and oddly healing.
WHAT I LEARNED
Illness teaches lessons that are practical, philosophical, and strangely social. Here are some of the things that stayed with me.
- Practical preparedness matters: Logistics—the small adaptions—make survival possible and dignified.
- Language shapes experience: Naming what's happening—central DI, desmopressin, sodium monitoring—turned fear into manageable tasks.
- Community is medicine: Friends, nurses, and the occasional stranger who offered a restroom changed outcomes in ways no pill could.
- Humor can heal: Choosing to wear a costume that made people smile didn't dismiss the seriousness of what I'd been through; it honored the fact that life could still hold joy.
PRACTICAL ADVICE FOR PATIENTS AND CAREGIVERS
The following are practical suggestions that blend medical sense with everyday habit changes. They are not medical instructions; your clinician is the final authority.
- Track intake and output: Keep a simple journal for a few days so clinicians can see patterns.
- Learn the symptoms of sodium imbalance: Confusion, severe headache, nausea, and seizures are urgent signs—seek help immediately.
- Carry identification: A small card explaining that you have DI and any medications helps in emergencies.
- Plan outings: Apps and websites can help locate restrooms, but simple forward planning—knowing where to stop—works too.
- Build a support team: An endocrinologist, an oncology nurse, and a trusted friend who knows your routines reduce decision fatigue.
CONCLUSION
The Halloween after treatment became a symbol: a public, slightly ridiculous punctuation mark on a private, arduous sentence. Wearing that costume felt like saying, loudly and clearly, "I am still here." More than the clothing or the label, what mattered was the reclamation of identity. Cancer and complications like diabetes insipidus roared through my life and rearranged it. They taught me about limits and resilience, about the mathematics of survival and the small mercies of community.
- Extreme polyuria can accompany brain conditions; it requires coordinated care with endocrinology and oncology.
- Practical adaptations—logistics, clothing, planning—are essential parts of living with chronic medical problems.
- Medication like desmopressin often helps manage central DI but must be used under medical supervision.
- Humor, ritual, and community are powerful aids in the recovery process.
There are days I still think in gallons—when a long meeting looms or when I plan a trip—but the fear that once ran like a river has been dammed into manageable streams. The costume was not a final note; it was an exclamation mark. I tell this story not for sympathy but because the way we live with illness is full of human invention. We invent pockets, habits, jokes, and costumes that help us walk back into the world. I walked back in, and every refillable bottle I carried was a reminder: survival can be practical, and it can also be absurdly, joyously celebratory.