Scientists Identify New Alzheimer’s Trigger — Drug That Blocks It
The headline reads like hope distilled: scientists say they have found a previously unrecognized trigger for Alzheimer’s disease and, remarkably, a drug that appears to block that trigger in laboratory models. If the findings hold, this is the kind of discovery that can redirect decades of research, alter how clinicians think about early detection, and — most urgently for millions of families — point to a path beyond symptomatic care toward disease modification. But between a laboratory breakthrough and a medicine that changes outcomes for patients lie careful validation, painstaking trials, and difficult clinical decisions. This feature unpacks what the discovery could mean, how the drug works in theory, and the practical hurdles ahead.
Alzheimer's disease brain research
Why this matters now
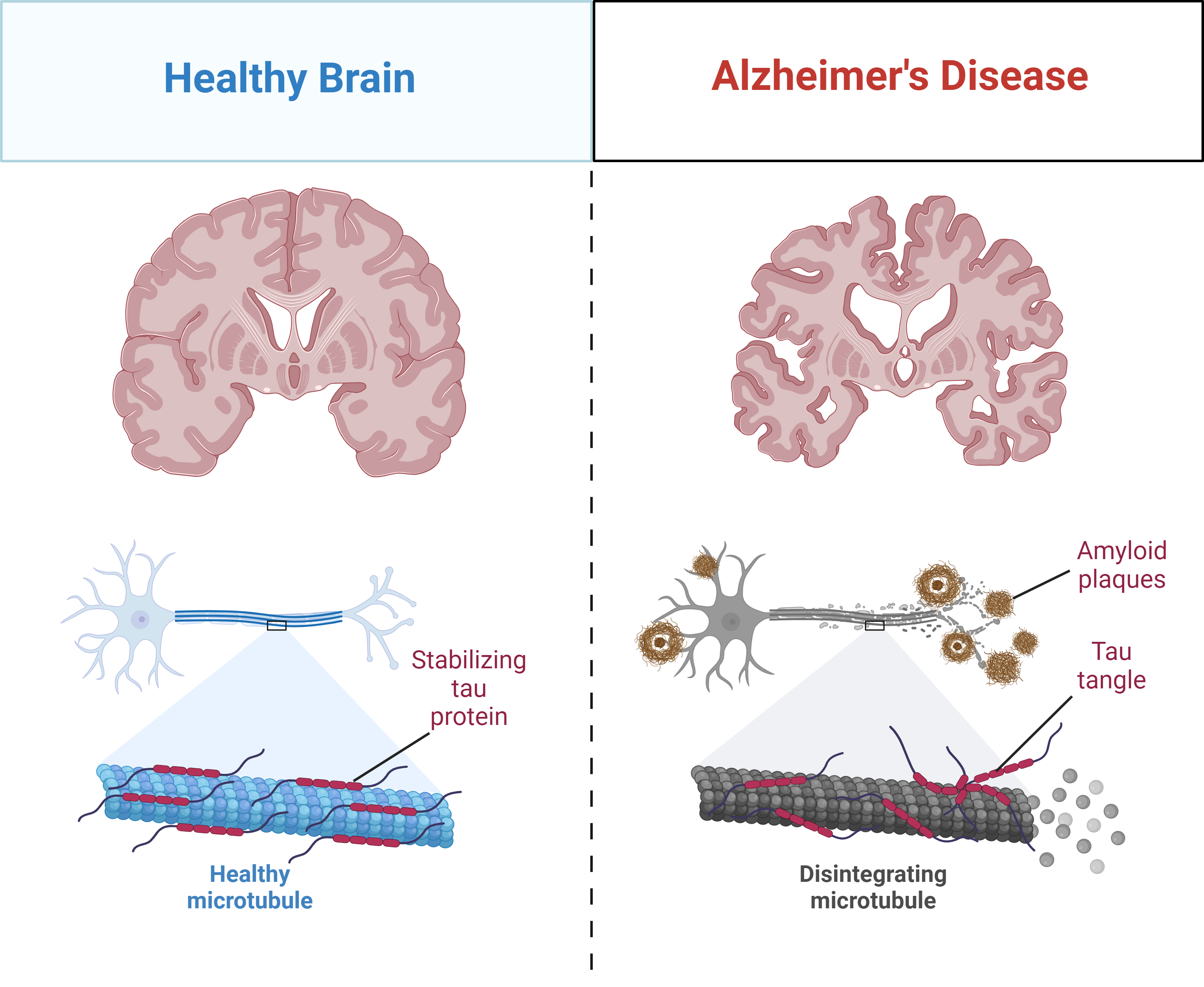
Alzheimer’s disease is not a single, uniform condition; it is a syndrome with multiple biological contributors that converge on memory loss, cognitive decline and, ultimately, loss of independence. For decades, researchers focused on two hallmark proteins — beta-amyloid and tau — and the plaques and tangles they form. Treatments aimed at clearing amyloid or slowing tau have had mixed success: some approaches modestly affect biomarkers, a few slow cognitive decline in selected patients, and many fail in late-stage trials. The central challenge has been that the processes leading to neuronal death are complex, stage-dependent, and sometimes downstream of earlier, subtler triggers. Finding an upstream switch — a trigger that sets off the cascade — is the kind of leverage point that could change prevention and treatment paradigms.
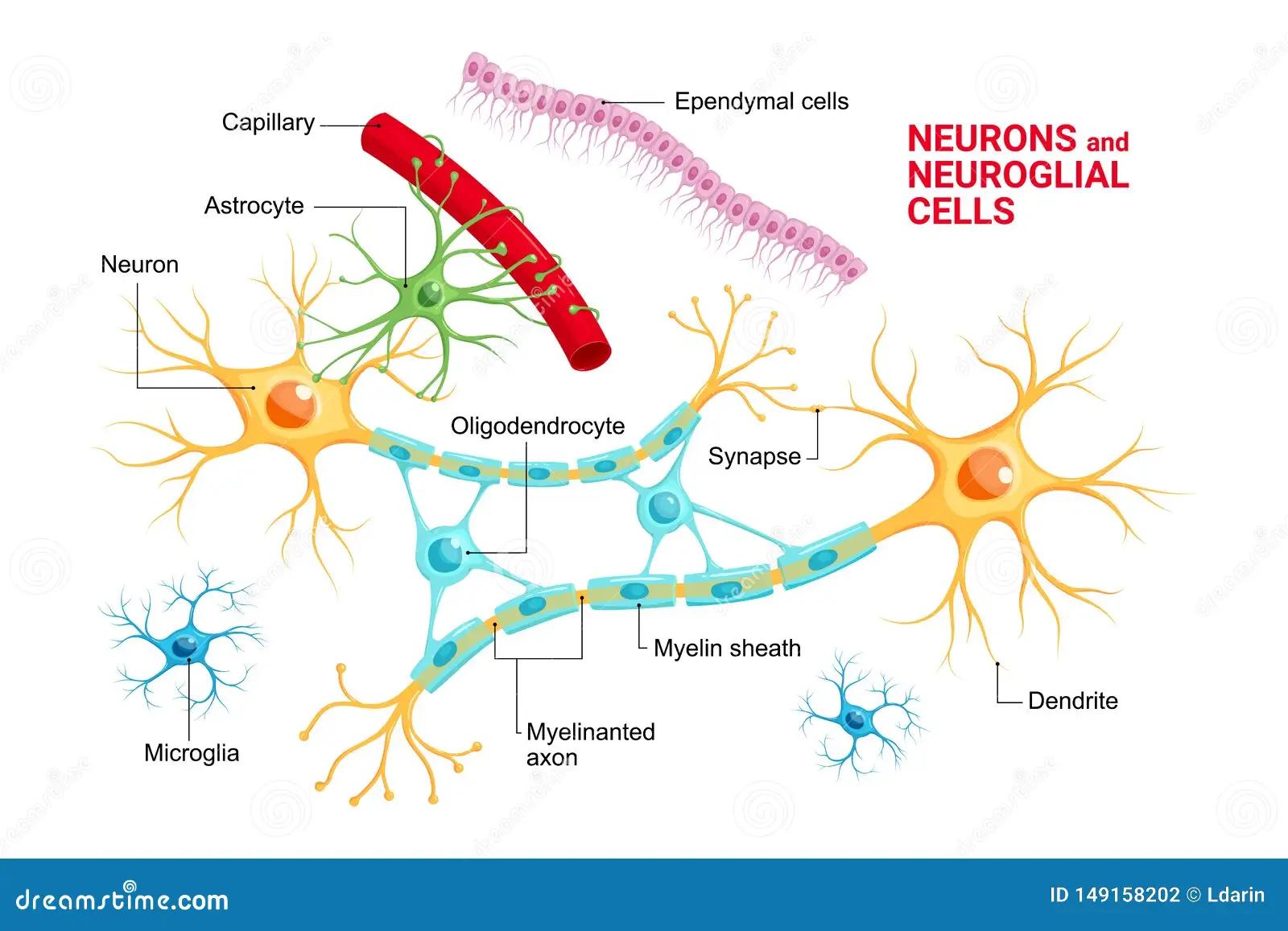
Microglia immune cells brain
The discovery: a new kind of trigger
What researchers reported
In the recent study, multidisciplinary teams identified a molecular cascade that had been overlooked because its components are transient and hard to measure in living tissue. The trigger lies at the intersection of cellular stress responses and innate immunity in the brain: a modified metabolic product produced by aging neurons that activates local immune cells (microglia), which then release factors that accelerate tau aggregation and synaptic pruning. The cascade strings together metabolism, immune activation, and protein misfolding — something like a match that lights the tinder of existing vulnerability in brain tissue.
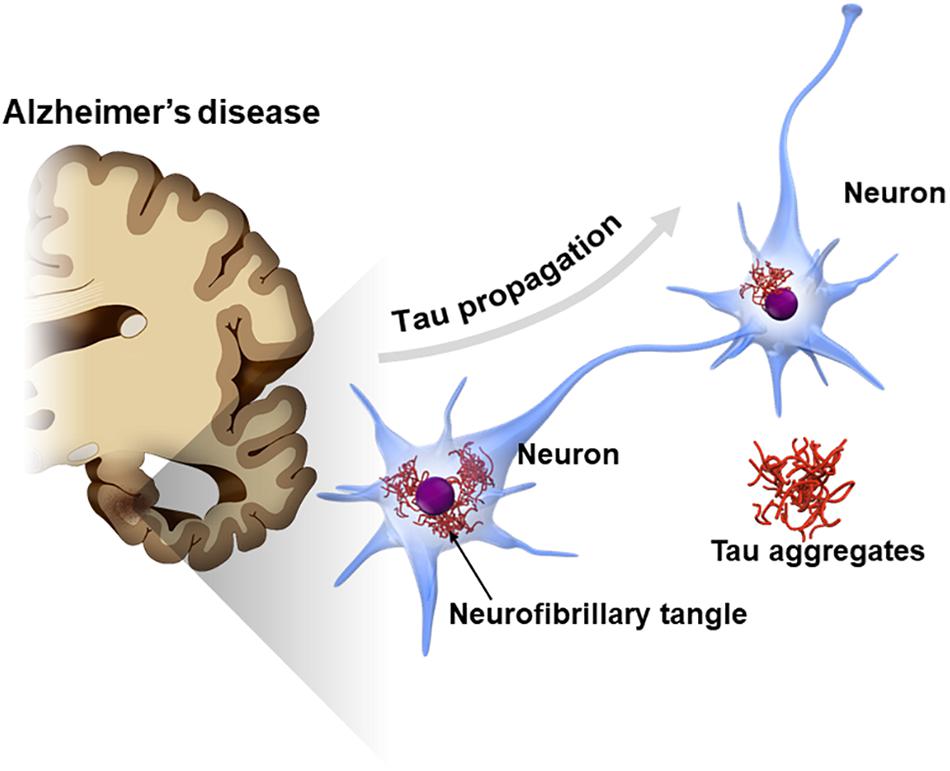
Tau protein aggregates Alzheimer's
How this differs from earlier models
Where amyloid-centric models posit that plaques are the initiating insult, this trigger behaves like a catalyst that accelerates tau pathology independently of plaque burden. That does not contradict amyloid theories; instead, it adds nuance. In some people, amyloid deposition may still matter most; in others — particularly late-onset cases or those with certain metabolic profiles — this newly described pathway could be the dominant driver. The discovery helps explain why some patients accumulate plaques without rapid cognitive decline, while others progress quickly despite modest amyloid load.
"A small metabolic whisper can become a thunderclap — and the drug we tested is meant to silence that whisper before it becomes noise."
The drug that stops the trigger
Mechanism of action
The candidate therapeutic is a small-molecule inhibitor designed to interrupt the chemical modification that converts a benign metabolite into the pro-inflammatory trigger. By blocking the enzyme or receptor responsible for that conversion, the drug prevents microglial overactivation and the downstream release of tau-seeding factors. Put simply: it targets an upstream switch rather than attempting to mop up damage once it has occurred.
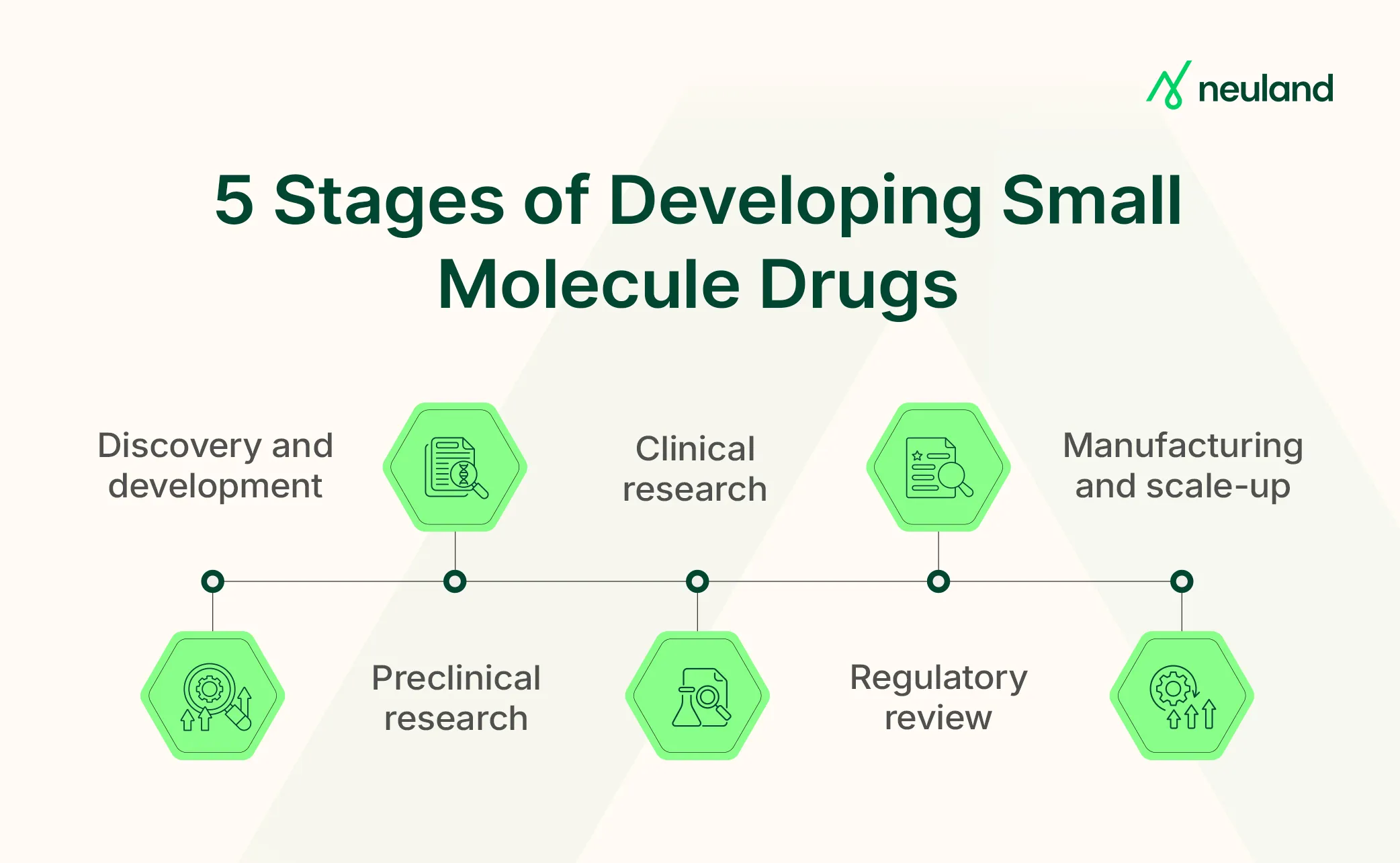
Small molecule drug development
Preclinical evidence
In animal models engineered to carry features of human Alzheimer’s pathology, researchers report that treatment with the drug reduced markers of microglial activation, diminished the formation of pathological tau aggregates, and preserved synaptic density and cognitive performance on maze and memory tasks. Importantly, the intervention was effective when started at an early symptomatic stage and, in some models, when administered before symptoms appeared — suggesting both therapeutic and preventive potential.
Why the approach is promising — and why caution is necessary
Potential advantages
The strategy offers several conceptual advantages:
- Broader impact: By acting upstream, the drug could influence multiple downstream pathologies (tau aggregation, synaptic loss) rather than a single protein species.
- Earlier intervention: If the trigger can be detected before extensive damage, the window for meaningful intervention widens.
- Complementary treatment: This approach could be combined with amyloid or tau therapies for additive benefits.
Important caveats
But early success in preclinical models is not uncommon and does not guarantee clinical benefit. Translational gaps include differences between animal and human immune responses, the complexity of human aging, and interindividual variation in the trigger’s role. Safety is another major concern: dampening immune responses in the brain risks impairing normal repair processes and infection control. Dose, timing, and patient selection will be critical variables.
"If we blunt microglia at the wrong time, we might remove a repair mechanism the brain needs."
Clinical implications and what to expect next
Path to clinical trials
Translating this discovery into treatments will require several steps: rigorous replication of the basic biology in human tissue and diverse populations, development of biomarkers to measure the trigger and on-target drug effects in patients, careful dose-ranging and safety studies, and then phased efficacy trials. Biomarkers are especially important because the trigger is transient and not visible on routine scans; researchers are developing blood and cerebrospinal fluid assays as well as PET ligands that might reveal pathway activation.
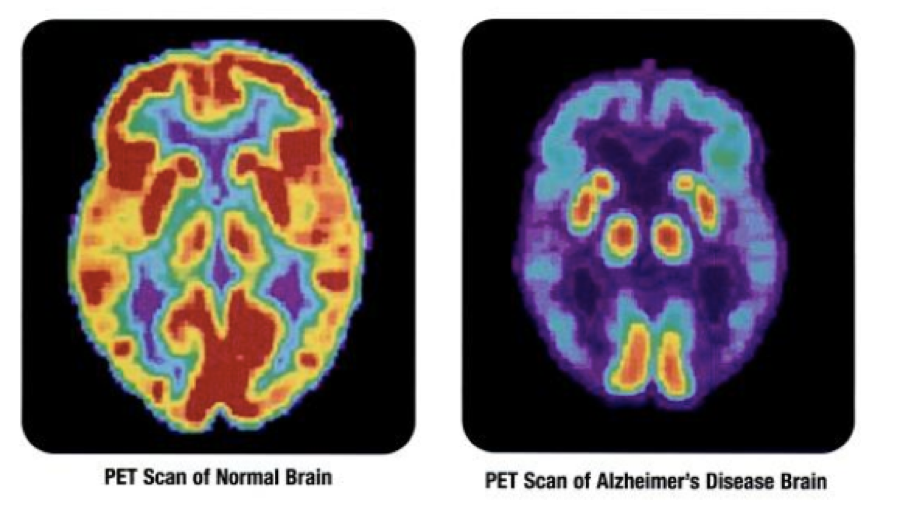
Brain PET imaging Alzheimer's
Who might benefit first
Initial trials will likely focus on people at high risk of progression: those with mild cognitive impairment, people with genetic risk factors, and volunteers in observational cohorts where longitudinal data and stored biomaterials allow researchers to test who expresses the trigger. If blood-based assays prove sensitive, the drug could eventually be tested in larger preventive trials in people with early biomarker signatures but no symptoms.
Ethics, equity and practical challenges
Breakthroughs invite ethical questions. If a blood test indicates a high risk of progression because the trigger is active, when should clinicians intervene? How will health systems pay for long preventive treatments? There is also the risk of widening disparities: early access to experimental diagnostics and drugs tends to concentrate in wealthier centers, leaving underserved populations behind. Researchers and policymakers must plan for equitable screening, trial recruitment, and, eventually, access to therapy.
Safety monitoring and long-term effects
Because the drug modulates immune activity in the brain, long-term safety monitoring will be essential. Potential adverse outcomes to watch for include increased susceptibility to infections, impairment of repair processes after stroke or trauma, and off-target systemic effects. Registries and long-term extension studies will be necessary to detect rare but serious harms.
"Safety over speed — the promise is huge, but the bar for altering brain immunity is appropriately high."
Broader scientific implications
This discovery reframes how scientists should think about the sequence of events that lead to neuronal loss. It pushes the field to integrate metabolism, immune signaling, and protein homeostasis into a single narrative rather than studying these processes in isolation. The idea that a small metabolic change can act as a trigger suggests new multidisciplinary avenues: epidemiologists can ask what lifestyle or environmental factors influence the metabolite; geneticists can search for variants that modulate susceptibility; and drug developers can design molecules that safely recalibrate the pathway.
Voices from the field
When a potential paradigm shift arrives, the research community responds with both excitement and skepticism. Some scientists welcome the fresh angle as a missing piece of the Alzheimer’s puzzle; others urge restraint until human data validate the mechanism. Clinicians emphasize the immediate need for therapies that improve patients’ daily lives and caution against overpromising to families already burdened by uncertain prognoses.
What patients and families should know
For people living with Alzheimer’s and their caregivers, headlines can raise hope and anxiety in equal measure. Here are practical points to keep in mind:
- Early-stage evidence: The drug’s effects are reported in laboratory and animal studies; clinical trials are the next step.
- Biomarker development: Detecting the trigger in humans is essential for identifying who might benefit.
- Complementary strategies: Lifestyle measures (sleep, exercise, cardiovascular health) remain important and may interact with the newly described pathway.
"Advances give hope, but they rarely replace the need for patience, monitoring, and supportive care in the near term."
Next steps and realistic timelines
If the discovery is replicated and biomarkers can be developed, the earliest clinical trials could begin within a few years. Phase 1 safety trials typically take a year or two, followed by larger Phase 2 trials to evaluate biological effect and dosing, and Phase 3 trials to test clinical benefit. Best-case scenarios are optimistic: a decade from discovery to approved therapy is fast; more commonly, the timeline stretches longer. That reality underscores the importance of parallel research: while this pathway is explored, continuing to refine symptomatic care and support services remains essential.
Conclusion
The discovery of a new trigger for Alzheimer’s disease and a candidate drug to block it is a major scientific moment. It reframes the disease as a dynamic interaction of metabolism and immunity, rather than a simple accumulation of misfolded proteins. The drug’s promise in preclinical work offers hope that intervening earlier and more precisely could alter disease trajectories. But the path from bench to bedside requires careful replication, biomarker validation, safety testing, and equitable trial designs. For now, the news renews a core lesson of Alzheimer’s research: the biology is complex, progress is incremental, and each credible advance brings us closer to therapies that meaningfully change lives.
- Researchers report a newly discovered molecular trigger that links metabolism and immune activation to accelerated Alzheimer’s pathology.
- A small-molecule drug that blocks the trigger showed protective effects in preclinical models, reducing tau aggregation and preserving cognition.
- Translating this finding to patients will require biomarkers, careful safety testing, and staged clinical trials; timelines are measured in years.
- Ethical and equity considerations must guide trial recruitment and eventual access to any approved treatment.