Russell's Viper Venom: How It Destroys Human Blood
The bite of Russell's viper is one of the clearest examples in nature of how a single biological cocktail can turn the most tightly regulated system in the body—blood coagulation—into a weapon against the host. In seconds to hours after envenoming, this venom can trigger both uncontrolled clotting and catastrophic bleeding, clog small vessels, damage kidneys, and leave survivors with long-term disability. Understanding what the venom does to human blood is not just academic: it is the difference between timely, life-saving treatment and preventable death.
Overview: Why Russell's Viper Is So Dangerous
Russell's viper (Daboia russelii and related species) lives in densely populated regions of South and Southeast Asia. Its venom is complex and highly active against the coagulation cascade. Unlike purely neurotoxic snakes, whose main threat is respiratory failure, Russell's viper delivers powerful hemotoxins that attack clotting factors, platelets, and blood vessels simultaneously. The result is a syndrome that can produce early clots, later bleeding, and organ damage—especially to the kidneys.

Russell's viper snake
A short clinical picture
After a bite, victims may notice local pain and swelling, but the true emergency often unfolds systemically: unexplained bleeding (from gums, nose, or puncture sites), dark or bloody urine, low blood pressure, and signs of kidney injury. In many cases laboratory tests show a dramatic fall in fibrinogen, prolonged clotting times, and platelet abnormalities.
"Russell's viper venom can both force blood to clot and render it unable to clot—sometimes in the same patient."
The Venom's Composition and How It Targets Blood
Venom is a complex mixture of proteins and enzymes. The key components relevant to blood are:
- Factor-activating enzymes: Some venom proteins directly activate human coagulation factors—most famously factors X and V, and in some venoms components that act like prothrombin activators. By shortcutting normal regulation, these enzymes create thrombin and fibrin very rapidly.
- Fibrinogen-degrading enzymes: Proteases that cleave fibrinogen into non-functional fragments or cause direct breakdown of fibrin, which reduces effective clot formation.
- Metalloproteinases and proteases: These damage vascular endothelium, increasing permeability and bleeding risk while also contributing to local tissue necrosis.
- Phospholipases A2 and platelet toxins: Molecules that impair platelet function and integrity, either promoting aggregation or causing platelet destruction depending on concentration and context.
coagulation factors illustration
The paradox: procoagulant then anticoagulant
One of the most striking features is the biphasic or simultaneous effect. Early, potent activation of clotting factors drives widespread generation of thrombin and the formation of fibrin—microthrombi that consume clotting proteins and platelets. As these substrates are used up, the blood loses the ability to clot when and where it is needed, producing severe bleeding. Clinicians call this pattern venom-induced consumptive coagulopathy (VICC); it resembles but is distinct from classic disseminated intravascular coagulation (DIC).
What Happens to the Blood—Step by Step
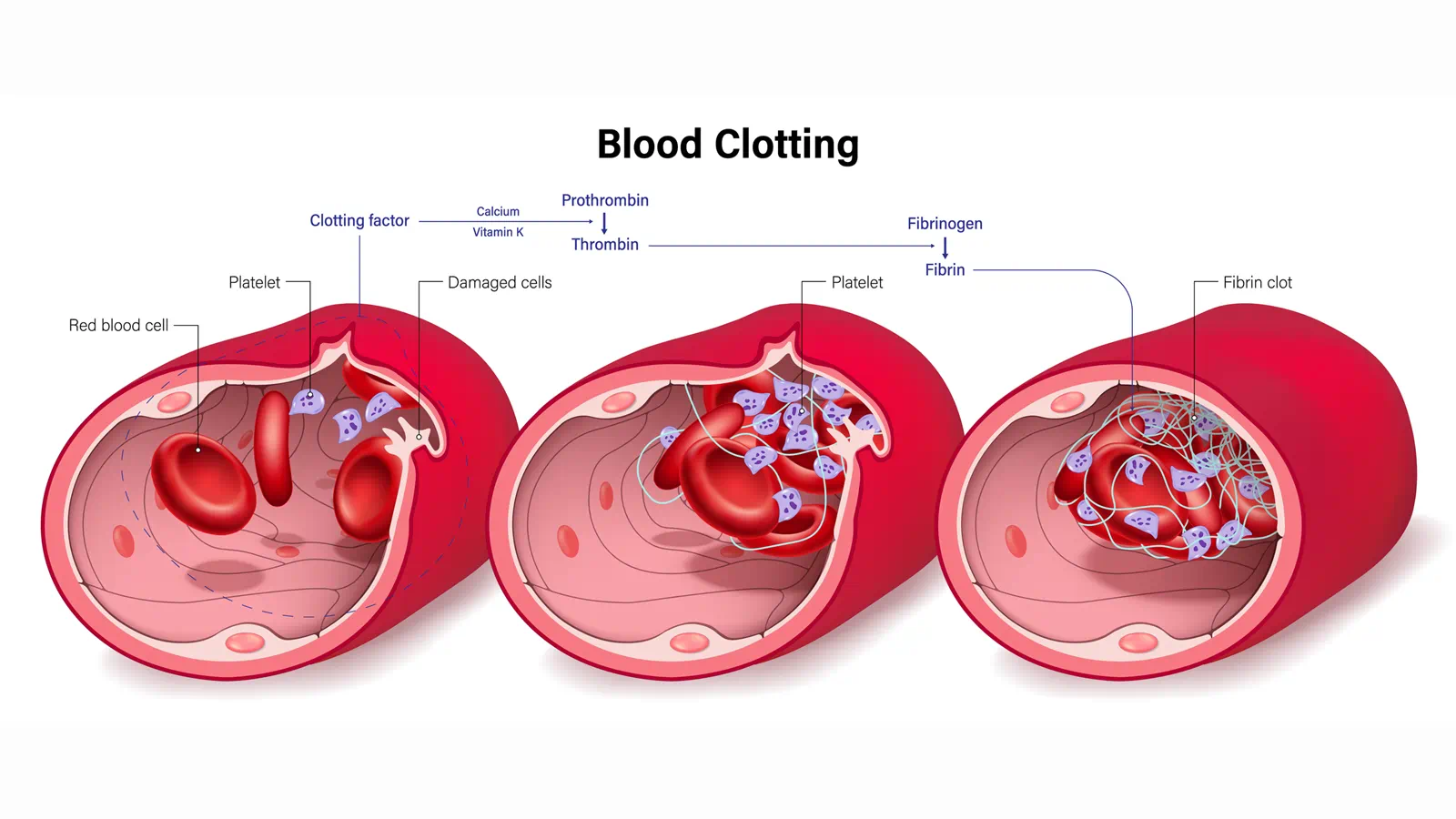
1. Immediate enzymatic activation of the clotting cascade
Venom factors that mimic or directly activate factor X/FV accelerate the conversion of prothrombin to thrombin. Thrombin converts fibrinogen to fibrin, producing clots in small vessels throughout the body. This process is often rapid and widespread.
2. Consumption of clotting factors and platelets
As fibrin forms in microvessels, fibrinogen levels fall and platelets become trapped or are destroyed. The laboratory picture begins to show low fibrinogen and low platelet counts. Blood loses its reserve of clotting potential.
blood coagulation diagram
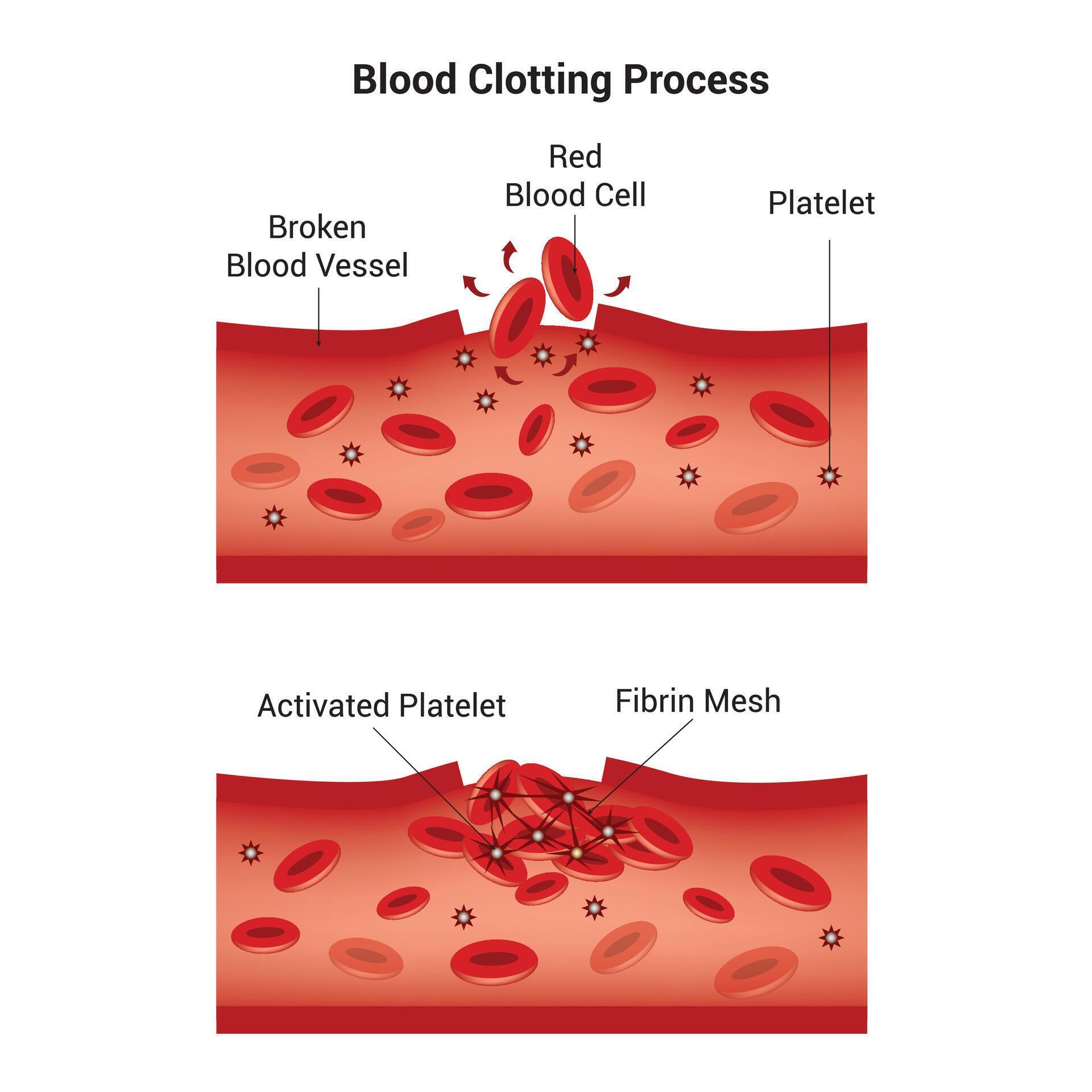
3. Fibrinolysis and breakdown of clots
Some venom enzymes stimulate fibrinolysis or produce fibrin degradation products. The result is an environment where clots are both forming and being broken down, creating a mess of small thrombi, degraded fibrin, and circulating fragments that impair further clot formation—worsening bleeding risk.
4. Endothelial damage and hemorrhage
Proteolytic venom components injure the lining of blood vessels, increasing leakage and local hemorrhage. Damaged endothelium also exposes tissue factor and collagen, promoting more clotting—in a vicious cycle.
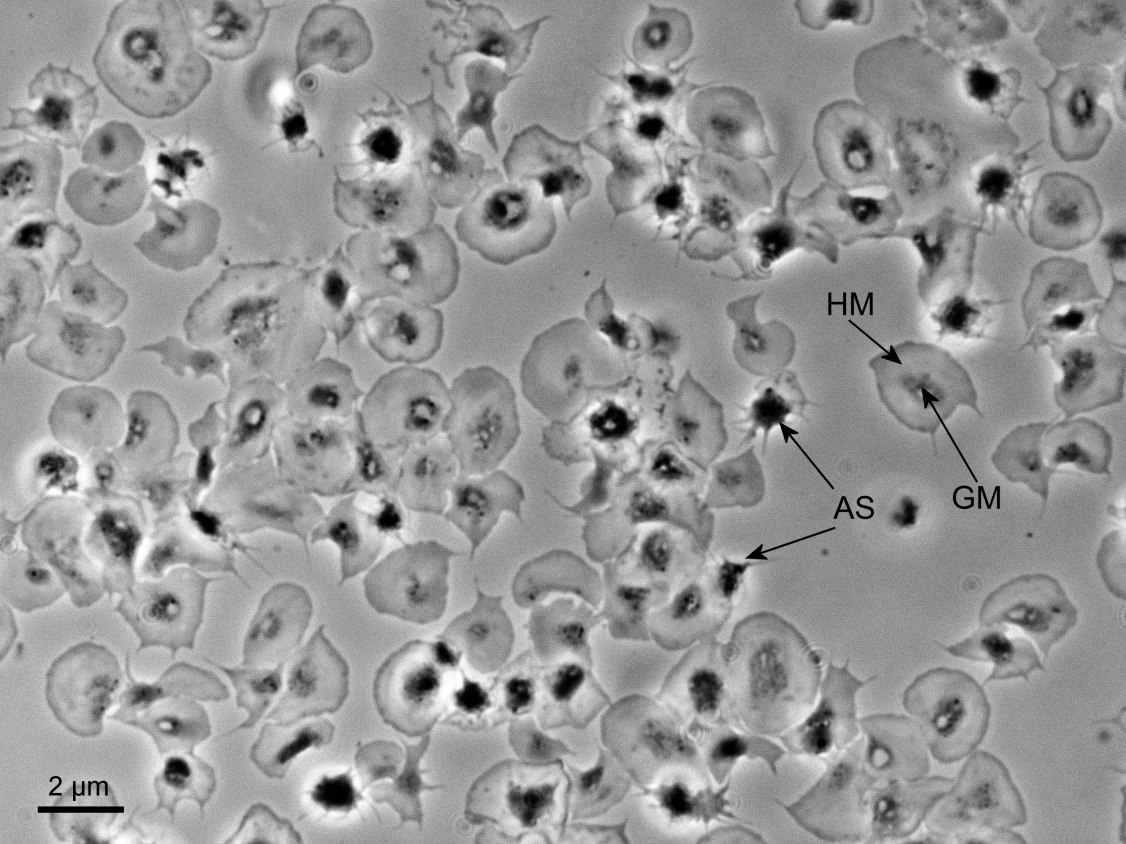
platelet aggregation microscopy
Clinical Signs and Laboratory Findings
Recognition depends on combining clinical clues with targeted labs.
- Common clinical findings: Local swelling and pain, bleeding from puncture sites or mucous membranes, hematuria (dark or red urine), hypotension, and signs of kidney impairment (reduced urine output, rising creatinine).
- Typical laboratory pattern: Low fibrinogen, prolonged prothrombin time (PT) and often prolonged activated partial thromboplastin time (aPTT), elevated fibrin degradation products (including D-dimer), thrombocytopenia, and sometimes anemia from bleeding or hemolysis.
- Coagulation profile: The most helpful test early is fibrinogen concentration; a falling fibrinogen is a red flag. Serial testing shows the dynamic nature: values can normalize after antivenom if treated promptly, or worsen if treatment is delayed.
Complications Beyond Bleeding
Blood abnormalities are the proximate cause of several dangerous organ complications.
Acute kidney injury (AKI)
AKI is common after Russell's viper bites. Mechanisms include microthrombi in renal vasculature, direct nephrotoxic effects of venom components, pigment nephropathy from hemoglobinuria or myoglobinuria, and hypotension. Clinically this can lead to oliguria or anuria and may require dialysis.
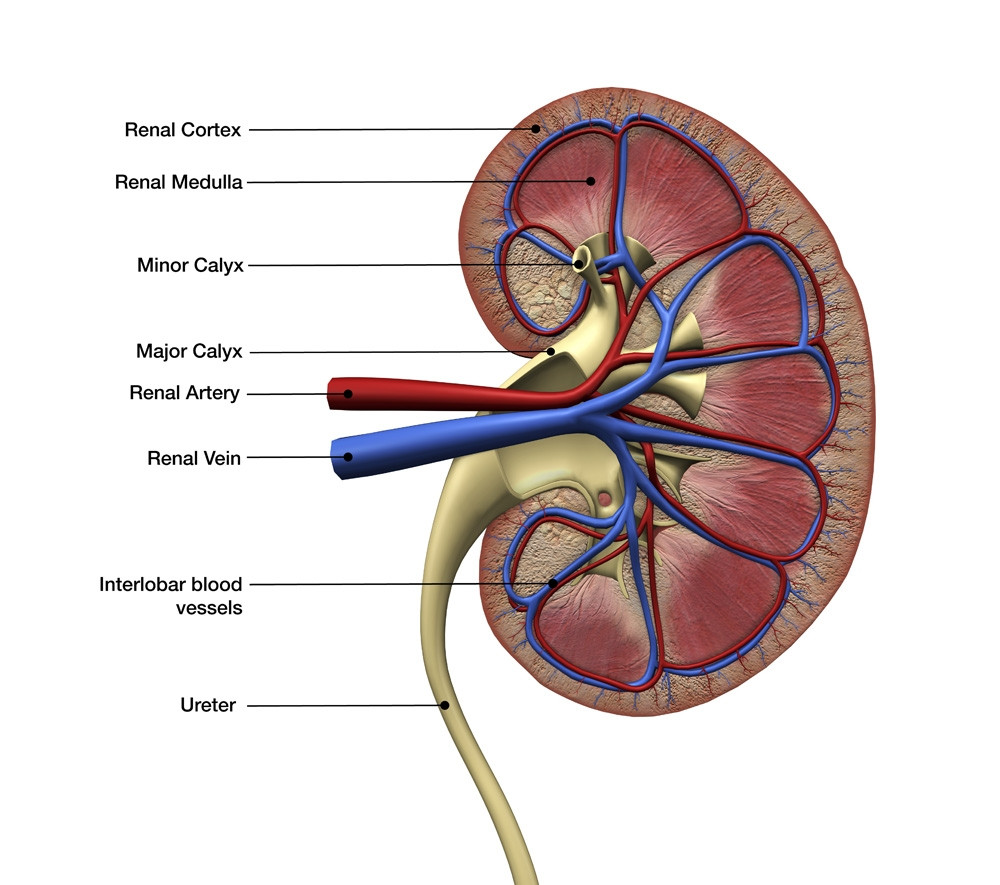
kidney anatomy cross-section
Thrombotic complications
Microvascular thrombosis can damage multiple organs. While large-vessel thrombosis is less common than bleeding, ischemic complications have been reported.
Local tissue loss and secondary infection
Proteases and metalloproteinases that damage vessels also destroy local tissue and can cause compartment syndrome, necrosis, and susceptibility to infection.
Diagnosis and Emergency Management
Immediate priorities
First aid and rapid transport to definitive care are the first line. In the hospital the immediate goals are to stabilize airway/breathing/circulation, establish IV access, and perform urgent labs (CBC, PT/INR, aPTT, fibrinogen, renal function, urine output).
Antivenom: the cornerstone
Specific antivenom for Russell's viper is the primary treatment. Antivenom contains antibodies that neutralize circulating venom components and halts further consumption of clotting factors. The effectiveness of antivenom is time-sensitive—early administration is associated with faster reversal of coagulopathy and fewer complications.
antivenom vial treatment
Supportive therapy
- Blood products: Fresh frozen plasma and cryoprecipitate can replace consumed clotting factors and fibrinogen when bleeding is severe or fibrinogen is critically low.
- Platelet transfusion: Consider when thrombocytopenia is profound and bleeding is uncontrolled.
- Renal support: Dialysis for AKI if indicated.
- Fluids and pressors: To maintain perfusion and limit kidney injury.
What to avoid
Routine use of antifibrinolytics or empiric aminocaproic acid is controversial and can be harmful if microthrombi predominate. Improper tourniquets, cutting the wound, or attempting to suck out venom are harmful first-aid measures.
Long-Term Outcomes and Rehabilitation
With timely antivenom and supportive care many patients survive without permanent disability. However, delayed treatment increases the risk of chronic kidney disease, amputations from local necrosis, and prolonged recovery from systemic organ injury. Rehabilitation may include physical therapy, wound care, and management of long-term renal insufficiency.
Public Health, Prevention, and Community Measures
Russell's viper bites are a preventable cause of death in rural regions. Public education about avoiding snake habitats, wearing protective footwear, storing food to discourage rodents (which attract snakes), and immediate transport to health facilities are effective strategies. Equally important is ensuring availability and supply of antivenom in regional hospitals and training healthcare workers in snakebite management.
Simple first aid checklist
- Do: Keep the patient calm, immobilize the bitten limb, remove tight jewelry, and transport to hospital quickly.
- Don't: Apply tight tourniquets, make local incisions, or try to suck venom out.
Key Takeaways and Practical Points
- Dual threat: Russell's viper venom triggers rapid clot formation that consumes clotting factors, then causes severe bleeding.
- Antivenom first: Specific antivenom given early is the most effective intervention to reverse coagulopathy.
- Watch kidneys: Acute kidney injury is common and may require dialysis.
- Lab monitoring: Serial fibrinogen, PT/INR, platelet count, and renal function guide therapy.
Conclusion: Respect, Rapid Response, and Research
Russell's viper venom is a masterclass in biological disruption of human physiology. It turns the coagulation system—normally a life-saving cascade—into a mechanism for self-destruction, with clotting and bleeding arising from the same pathological processes. The good news is that this biochemical assault can be countered: antivenom neutralizes circulating toxins, targeted supportive care manages complications, and prevention reduces incidence. Continued public health work to expand access to antivenom, clinician training in rural hospitals, and research into improved therapies remain essential if we are to reduce the toll of this dangerous envenoming.
Timely treatment transforms venom from a death sentence into a survivable medical emergency.