Rare Skin Cancer Mistaken for Vitamin Deficiency for 8 Years
The first time Maria noticed it, she blamed the sun. A faint, scaly patch on her chest—reddish, dry, uncomfortable—came and went with seasons. Over the next eight years the patch multiplied: other areas reddened, flaked, and itched. Her primary care doctor prescribed topical creams and suggested dietary changes and supplements. A nutrition-focused diagnosis—vitamin deficiency—felt comforting and simple. It explained a mysterious skin problem without immediate alarm. Eight years later, a referral to a dermatologist and a third biopsy revealed a diagnosis no one had expected: a rare form of skin cancer that masqueraded as a deficiency for nearly a decade.
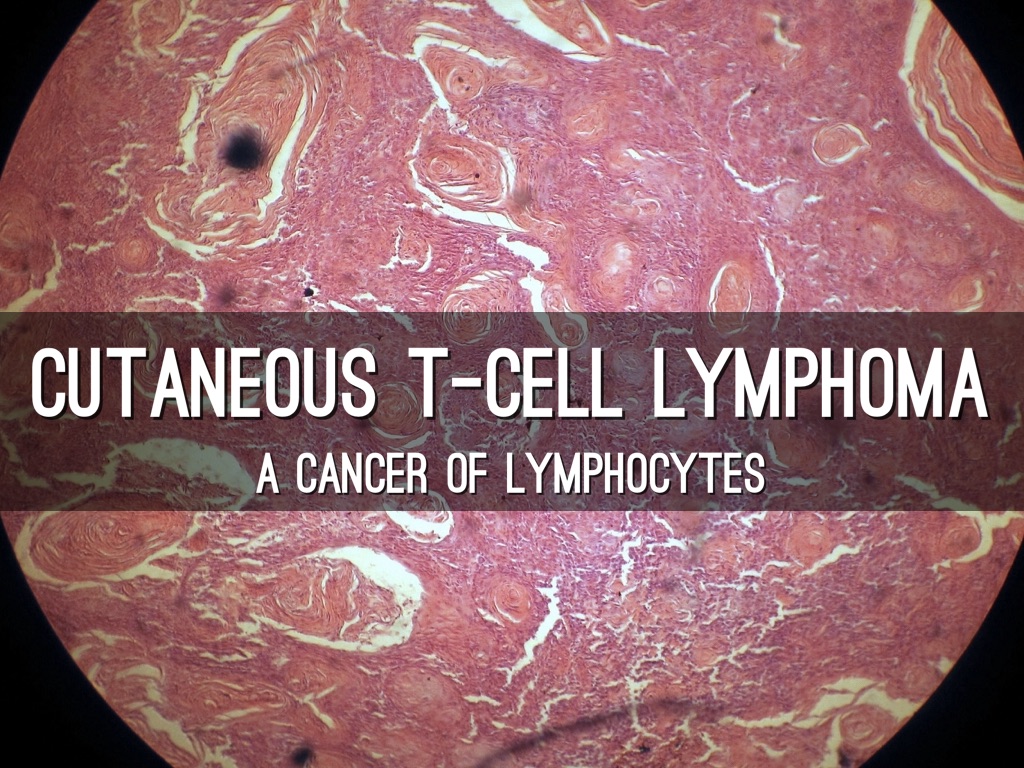
cutaneous T-cell lymphoma
A Rash That Would Not Quit
Chronic skin problems are common. Many are benign and respond to creams, moisturizers, improved diet, or time. That’s precisely why serious conditions that look similar can slip through the cracks. Maria’s initial symptoms—patchy discoloration, scaling, intermittent itching—overlapped with several benign explanations. Her doctors saw what most clinicians see every day: eczema, contact dermatitis, perhaps a nutritional skin change. She was treated accordingly. The problem, however, didn’t resolve.
“It was easy to normalize the rash because it behaved like so many harmless things.”

mycosis fungoides
When Vitamin Deficiency Became the Default Diagnosis
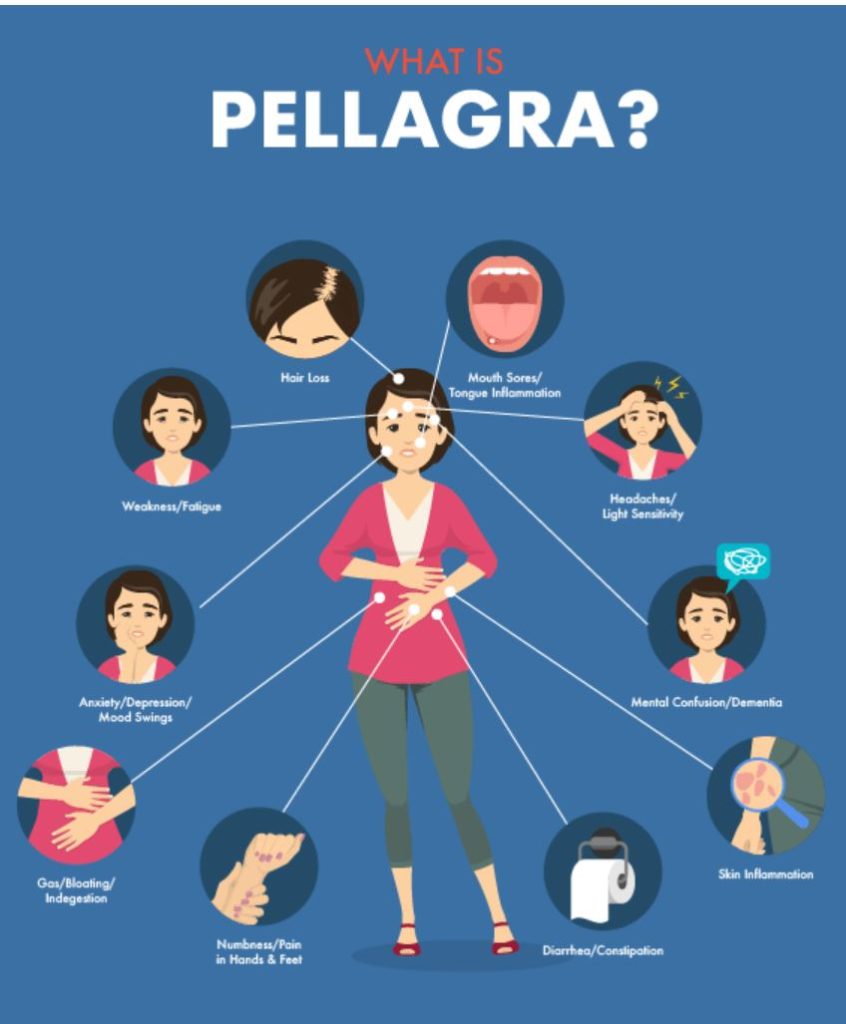
When primary care clinicians or even dermatologists encounter nonspecific photosensitive or scaly rashes, nutritional deficiencies—particularly niacin (vitamin B3) deficiency, known as pellagra—are part of the differential. Pellagra causes a classic photosensitive dermatitis in sun-exposed areas, sometimes with hyperpigmentation and scaling, and when physicians see that pattern they may advise supplements, dietary changes, or sun protection. For many patients, that advice helps. For others, it delays the deeper workup that could reveal a different cause.
There are a few practical reasons this happens:
- Symptom overlap: Early-stage skin cancers, certain inflammatory diseases, and nutritional dermatoses can look nearly identical under casual inspection.
- Response to treatment: Short-term improvement with topical steroids or improved nutrition can create false reassurance even when the underlying process persists.
- Variable biopsy findings: Early or subtle malignancies sometimes yield nondiagnostic biopsy results, or pathologic features can be read as chronic dermatitis by a nonspecialist.
The Hidden Culprit: Cutaneous T-Cell Lymphoma
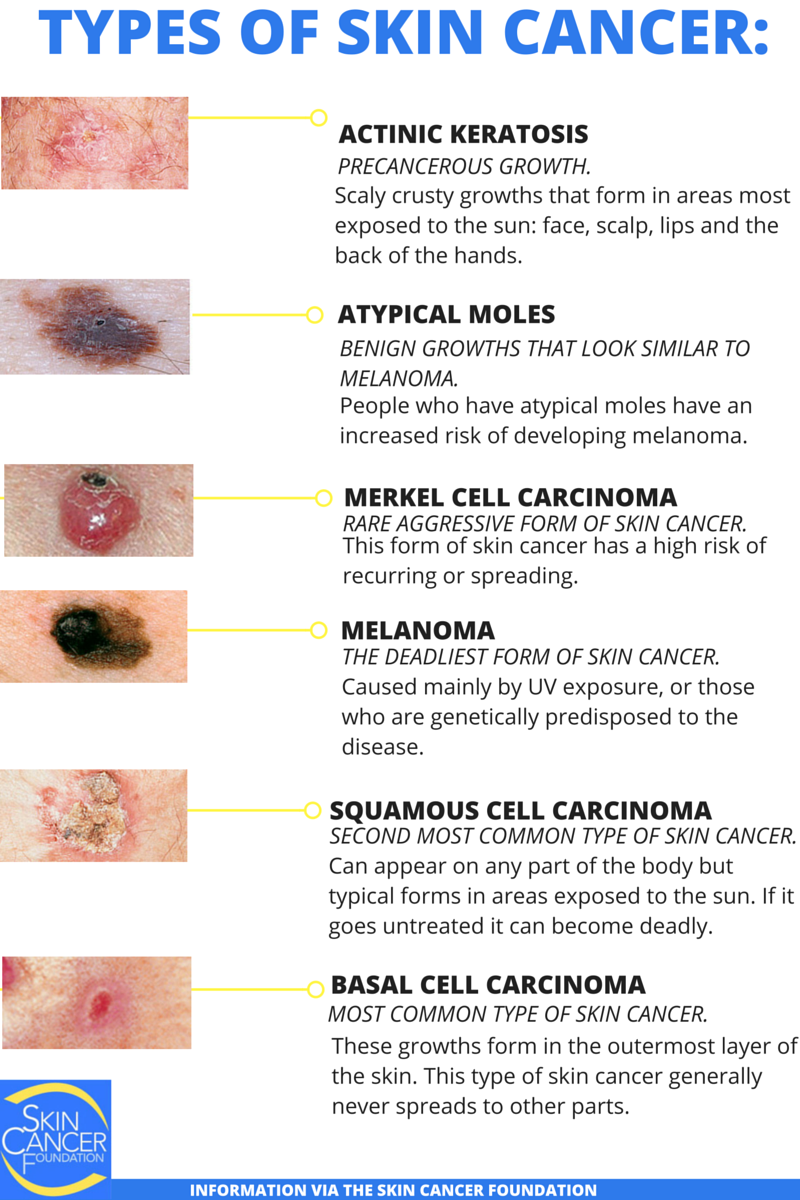
One of the conditions most notorious for masquerading as chronic eczema or nutritional dermatitis is cutaneous T-cell lymphoma (CTCL), with mycosis fungoides (MF) being the common clinical variant. This is not the same as melanoma or the more familiar squamous cell or basal cell carcinomas. CTCL is a lymphoid malignancy—cancer of T cells—that primarily affects the skin and can evolve slowly over years or decades. Its early stages are often indistinguishable from benign inflammatory conditions.
skin biopsy dermatology
Patients with early MF present with patches or plaques—red, scaly, and sometimes itchy lesions—that wax and wane. They can respond partially to topical therapies, further confounding clinicians. Only when the disease progresses or when specialized tests are performed does the diagnosis become clear.
Why It's So Often Missed
Delays in diagnosing rare skin cancers like CTCL arise from a constellation of factors. Understanding these helps both patients and clinicians know when to dig deeper.
- Subtle histology: Small biopsies can show nonspecific chronic inflammation. Pathologists with limited dermatopathology experience may interpret these findings as dermatitis rather than malignancy.
- Sampling error: A single biopsy may not capture diagnostic tissue. Multiple biopsies from different sites and at different disease stages may be required.
- Clinical mimicry: Nutritional disorders, autoimmune rashes, chronic infections, and even drug reactions can produce similar clinical pictures.
- Therapeutic masking: Repeated steroid courses can modify the appearance of lesions and alter biopsy features, delaying recognition.

photosensitive dermatitis rash
How Diagnosis Finally Happened
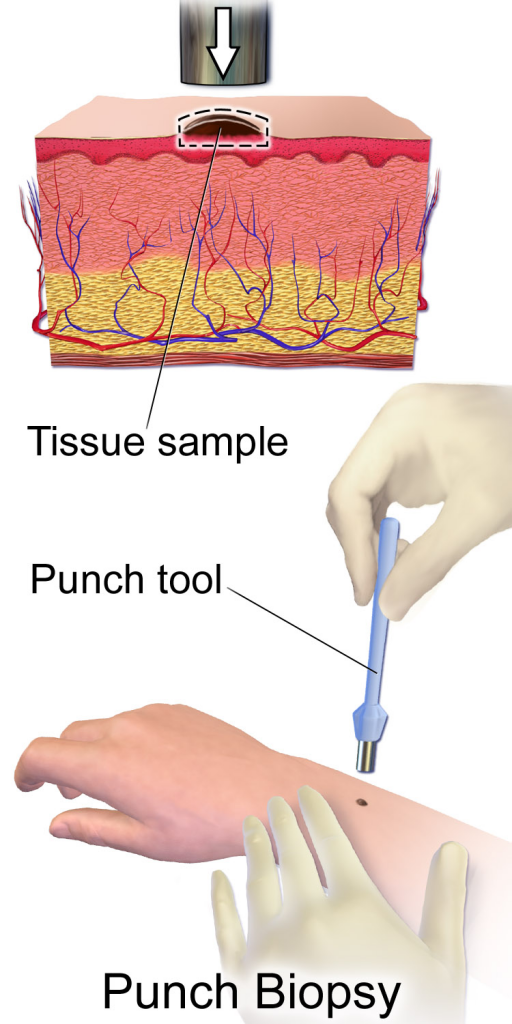
In Maria’s case the turning point came during a specialist visit. The dermatologist listened differently: she mapped the distribution of lesions, took a careful history of waxing and waning, and ordered multiple targeted biopsies. The pathology laboratory used special stains and immunophenotyping that revealed atypical T cells, and molecular testing showed a clonal T-cell receptor rearrangement—consistent with mycosis fungoides.
vitamin deficiency pellagra
Key diagnostic steps that often reveal these hidden cancers include:
- Repeat biopsies: Sampling different lesions and repeating biopsies over time increases yield.
- Dermatopathologist review: Expert interpretation is crucial; dermatopathologists evaluate patterns that general pathologists may miss.
- Immunohistochemistry and molecular testing: These tools identify aberrant cell populations and clonality that point to lymphoma rather than benign inflammation.
Treatment: From Skin Care to Systemic Therapy
Once diagnosed, the treatment strategy depends on disease stage and patient goals. CTCL and MF have a spectrum of therapies—from gentle skin-directed treatments suitable for early-stage disease to systemic agents for more advanced disease. Many patients do well for years with treatments designed to control symptoms and slow progression.

chronic scaly skin patch
Common approaches include:
- Topical therapies: Steroids, retinoids, or targeted topical chemotherapies can reduce lesions in early disease.
- Phototherapy: Controlled ultraviolet light treatment is effective for many patients with widespread patches or plaques.
- Systemic options: For more advanced disease, oral retinoids, interferon, targeted monoclonal antibodies, or other systemic therapies may be considered.
- Procedural therapies: In localized tumors or thicker plaques, surgery or radiation can be appropriate.
Importantly, treatment is often a balance between disease control and quality of life. Because the disease can be indolent, aggressive therapies are reserved for those who truly need them.

dermatopathologist review
The Emotional Toll of a Slow Diagnosis
Being told for years that a problem is nutritional or benign when it’s not has emotional consequences. Patients like Maria report frustration, anxiety, and a fragile trust in the medical system. They may feel guilty for having pursued supplements or for not insisting on referrals. A late cancer diagnosis can reopen wounds and raise questions about whether earlier intervention would have changed the outcome.
Health care teams must address not just the physical disease but the emotional aftermath: clear explanation, a shared plan, and validation of the patient’s perseverance are important parts of the healing process.
What Patients Should Watch For
Most rashes are harmless, so the goal is not to create unnecessary alarm but to arm patients with practical criteria to prompt a second opinion. Consider further evaluation if you notice any of the following:
- Persistent lesions: Rashes that do not clear after adequate topical therapy and time.
- Change in character: New thickness, scale, or nodularity in a lesion that was flat.
- Distribution that defies explanation: Lesions appearing in non–sun-exposed areas or in a symmetrical, widespread pattern.
- Treatment resistance: Recurrence despite appropriate therapy or partial/temporary improvement only.
- Systemic symptoms: Unexplained weight loss, fevers, or night sweats (less common but important).
Advice for Clinicians
Primary care clinicians hold a critical gatekeeper role. Most skin problems are benign, but a high index of suspicion should be maintained when clinical response is incomplete or when histology is equivocal. Practical steps include:
- Document and map lesions: Photographs and body maps improve longitudinal assessment.
- Coordinate with dermatopathologists: When biopsy results are ambiguous, discuss the case with a specialist.
- Repeat and diversify sampling: Take multiple biopsies from representative lesions at different stages.
- Refer early: A dermatology consultation is low-risk and can prevent long diagnostic delays.
phototherapy for skin cancer
A Broader Look: Why Diagnostic Delays Happen Systemically
The medical system itself creates environment where slow-progressing, rare diseases are often discovered late. Limited access to specialists, variable insurance coverage for advanced testing, and uneven familiarity with rare dermatologic malignancies across clinicians contribute. Improving education in primary care, expanding access to dermatology and dermatopathology expertise, and developing clear referral pathways are systemic solutions that pay dividends in earlier detection.
Real-World Outcomes and Hope
Many patients with early-stage CTCL do very well. Treatments control symptoms, and with modern therapies clinicians can offer targeted options aimed at preserving quality of life. Even for those with more advanced disease, advances in immunotherapy and targeted agents have widened the therapeutic toolkit. The key determinant of outcome, however, is timely diagnosis: the sooner the disease is correctly identified, the sooner patients can receive the most appropriate care.
Conclusion: Listening, Testing, and Persistence Matter
Maria’s eight-year journey from presumed vitamin deficiency to confirmed diagnosis is a cautionary tale and a human one. It shows how reasonable initial assumptions, partial treatment responses, and the limitations of early biopsies can conspire to delay recognition of a rare but important cancer. It also shows the power of persistence—patients who keep advocating, clinicians who listen, and specialists who apply focused testing can change a trajectory.
For patients: if something about your skin isn’t right and it doesn’t resolve, you have the right to ask for a second opinion, a referral, or repeat testing. For clinicians: maintain humility in the face of diagnostic uncertainty—repeat biopsies and specialist input are not admissions of failure but prudent clinical care. Together, thoughtful listening, careful testing, and attentive follow-up can make sure that a treatable condition is not hidden behind a convenient explanation.
- Rare skin cancers like cutaneous T-cell lymphoma can imitate benign conditions including vitamin deficiency for years.
- Repeat biopsies, dermatopathologist review, and molecular testing increase diagnostic accuracy.
- Persisting or changing rashes deserve referral; early diagnosis improves management options and quality of life.
Patient name changed and details condensed to protect privacy; medical descriptions are generalized for educational purposes.