
New Oral Weight-Loss Pill Outperforms Ozempic in Major Trial
In a development that could reshape the landscape of obesity treatment, a newly tested oral weight-loss pill has demonstrated superior efficacy to an oral formulation of semaglutide—often associated with the brand Ozempic—in a large randomized clinical trial. The result, described by investigators as both clinically meaningful and potentially practice-changing, opens a conversation about convenience, adherence, and how best to match therapies to patients with obesity and related metabolic conditions.

oral weight loss medication
"Efficacy is only one part of the story; delivery, patient preference, and safety together determine whether a therapy will change practice."
Why this matters now
The modern treatment era for obesity has been transformed by a class of medications called GLP-1 receptor agonists and related incretin-based therapies, which reduce appetite, slow gastric emptying, and change energy balance in ways that produce sustained weight loss for many people. Until recently, the most visible successes were injectable drugs; the arrival of oral formulations expanded the field. A new pill that outperforms an existing oral GLP-1 option raises the possibility of broader accessibility and greater patient choice, particularly for people who dislike injections or who struggle with adherence to weekly or daily injectable regimens.
semaglutide Ozempic medication
The trial at a glance
The trial was a randomized, controlled, multi-center study enrolling thousands of adults with overweight or obesity. Participants were assigned to receive either the new oral pill, an oral formulation of semaglutide used as a comparator, or placebo, and were followed for a year with standardized lifestyle counseling across arms. Primary endpoints focused on percent body weight change and the proportion of participants achieving clinically relevant thresholds of weight loss (for example, 10% or greater).
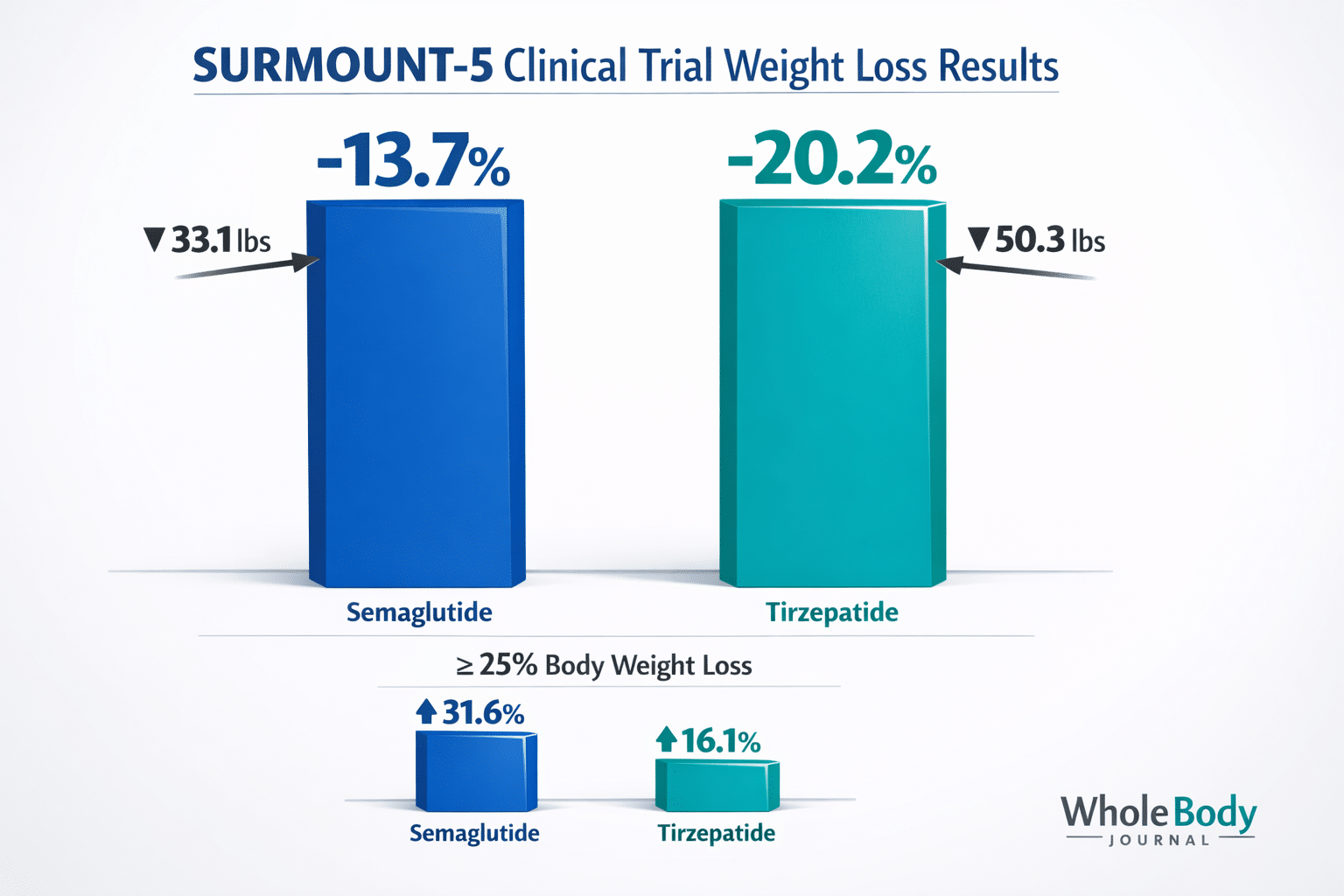
clinical trial weight loss
Investigators reported that the investigational medicine produced a statistically greater average percentage weight loss compared with the oral semaglutide group and markedly outperformed placebo. Importantly, the trial included broad eligibility—people with and without type 2 diabetes, varied baseline body mass indices, and a range of ages—improving generalizability to typical clinical populations.
Understanding the mechanisms—what might explain the difference?
Pharmacology provides plausible reasons a new oral agent could outperform an existing oral GLP-1 formulation. Differences in molecular design, receptor affinity, dual-agonist activity (targeting GLP-1 plus GIP or glucagon pathways), and improved oral bioavailability can translate into larger effects on appetite regulation, energy expenditure, and glycemic control. Formulation technology—how the drug survives digestion and is absorbed—also matters with oral peptide drugs, historically a difficult challenge.
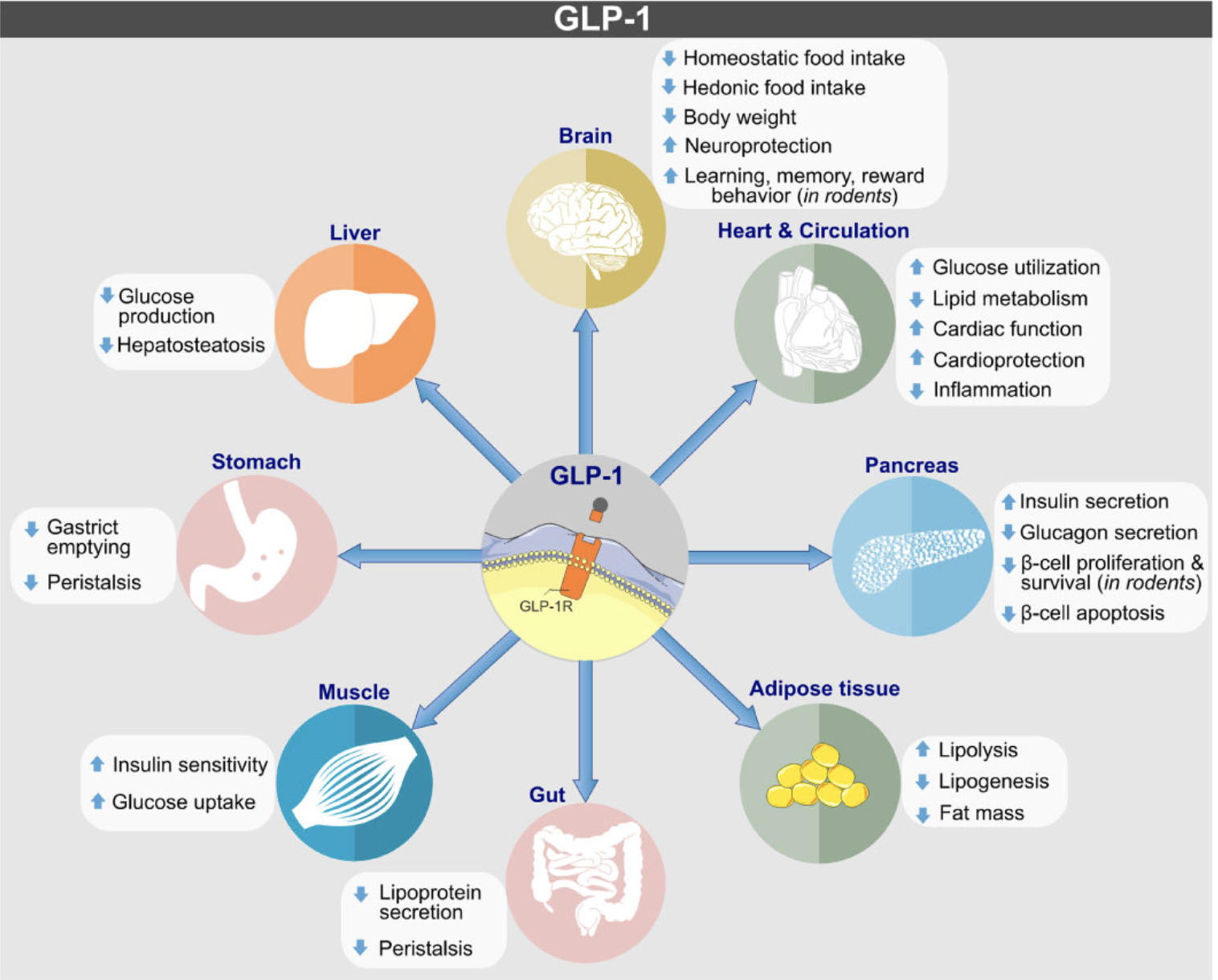
GLP-1 receptor agonist
While oral semaglutide represented a breakthrough by delivering a peptide orally, the new pill appears to combine improved receptor signaling with formulation advances that maintain therapeutic blood levels more consistently. Longer duration of action, fewer peaks and troughs, and combined receptor activity could together explain greater average weight reduction observed in the trial.
What the numbers mean for patients
For patients, the most tangible measure is the amount of weight lost and how that translates into improvements in blood pressure, glucose control, mobility, and quality of life. In the trial, a larger share of participants on the new pill reached clinically significant weight-loss milestones compared with those on the oral semaglutide arm. Clinically significant thresholds—commonly 5%, ইন%, and 15% weight loss—are associated with incremental improvements in cardiometabolic risk factors; therefore, more participants clearing those thresholds means potentially greater population-level benefits.
But raw percentages don’t tell the full story. Side effects, tolerability, and how a drug affects daily life are crucial. Gastrointestinal symptoms such as nausea and diarrhea are common across GLP-1–based therapies; the trial reported tolerability profiles that were broadly similar between the two oral agents, though some differences in frequency and severity were noted. Safety monitoring also included standard cardiovascular endpoints and lab assessments relevant to liver and kidney function.
Adherence, accessibility, and the psychology of a pill
One of the most disruptive aspects of an effective oral therapy is its potential effect on adherence. Studies of chronic medications repeatedly show that patients prefer oral pills over injections, and adherence is often higher when a medication fits more naturally into daily routines. For obesity—where lifetime management is commonly necessary—ease of use can determine whether a therapy delivers sustained benefit.

obesity treatment clinic
Beyond convenience, there’s a psychological element. Some patients resist or delay injectable treatments long enough that their health deteriorates. An effective oral option can lower that barrier. It also may change how primary care clinicians discuss weight management, making pharmacotherapy a more approachable step alongside nutrition counseling and physical activity guidance.
Safety profile and monitoring
Any discussion of a new anti-obesity medication must weigh efficacy against safety. Common adverse events for incretin-based therapies include gastrointestinal symptoms, transient increases in heart rate, and potential effects on gallbladder function. The trial reported adverse event rates consistent with this class, but also described differences worth noting for prescribers: rates of discontinuation due to intolerability, specific symptom patterns, and laboratory changes were all quantified and compared between groups.
Regulatory bodies will pay particular attention to rare but serious events, and post-marketing surveillance will be essential to detect outcomes that are too uncommon to appear in pre-approval trials. Practicing clinicians should expect guidance on patient selection, baseline testing (for example, liver and kidney function), and monitoring schedules if the drug advances toward approval.
How this fits with other available treatments
Obesity treatment is not one-size-fits-all. Clinicians today select from lifestyle programs, behavioral therapy, pharmacotherapy, and bariatric surgery depending on severity, comorbidities, and patient preference. The addition of a more effective oral agent expands the mid-tier of options—potentially offering substantial weight loss without the invasiveness of surgery and with greater convenience than injections.
medical pill comparison
- Oral administration — improved convenience and potential adherence.
- Greater average weight loss — more patients reaching meaningful thresholds.
- Broad eligibility — trial included people with and without diabetes.
- Unknown long-term safety — outcomes beyond trial duration remain to be seen.
- Cost and access — new branded therapies can be expensive and face insurance hurdles.
- GI side effects — comparable adverse events may limit tolerability for some.
Implications for clinicians and health systems
Clinicians will want to understand relative benefits for individual patients: who gains the most, who tolerates it best, and how to sequence therapies. Health systems and payers will rapidly ask questions about cost-effectiveness: how many cardiovascular events, diabetes cases, or surgeries might be avoided by wider use of an efficacious oral medication? Economic models built from trial outcomes and real-world data will guide coverage decisions.
Primary care providers could be the front line for prescribing and managing patients on this therapy, making education and clear clinical pathways essential. Endocrinologists, cardiologists, and bariatric specialists will also play roles for more complex patients or those with significant comorbidities.
What patients should ask their doctors
Patients hearing about this trial should approach conversations with clinicians prepared and pragmatic. Useful questions include: Am I a candidate for this therapy? How does it compare to other options I might use? What side effects should I expect, and how will they be managed? What monitoring will be necessary? If cost is a concern, what support programs or coverage options are available? Such conversations are best framed within a long-term plan that includes nutrition, physical activity, and behavioral support.
Equity and access: a major concern
New medications that promise meaningful weight loss risk widening disparities if they are expensive, poorly covered by insurance, or unavailable in resource-limited settings. The history of novel therapeutics shows that cost and distribution determine who benefits. Policymakers, payers, and manufacturers will need to grapple with pricing strategies, patient assistance programs, and equitable distribution to ensure the public-health potential of a superior oral therapy is realized broadly rather than concentrated among those with the best resources.
Real-world questions that remain
Randomized trials set the standard for efficacy, but real-world effectiveness can differ. Key questions for the post-trial period include: How will patients fare outside the closely monitored environment of a study? What are adherence patterns over multiple years? How does the medication interact with commonly used drugs? And what is the experience among populations often underrepresented in trials, including those with multiple comorbidities, older adults, and certain racial and ethnic groups?
Researchers and clinicians will also be watching whether weight regain occurs after treatment cessation, and how long treatment must be continued to maintain benefits. The answers will shape guidelines and inform decisions about starting, continuing, or stopping therapy.
A note on lifestyle and comprehensive care
Even the most effective pharmacologic tools work best when paired with lifestyle support. Nutrition counseling, physical activity, sleep hygiene, and behavioral therapy remain core components of sustained weight management. An oral medication that improves the capacity to engage in healthy behaviors—by reducing hunger and improving energy—can be a powerful adjunct, but it is not a standalone solution for the broad societal challenge of obesity.
"Medication plus systems of care—behavioral support, community programs, and policy change—unlock the real public-health impact of new therapies."
Conclusion: cautious optimism
The trial comparing a new oral weight-loss pill with an oral formulation of semaglutide yields cause for cautious optimism: greater average weight loss, broader convenience, and the possibility of improved adherence. Yet important caveats remain—long-term safety, real-world effectiveness, cost, and equitable access will determine whether this development translates into improved population health.
For clinicians and patients, the message is pragmatic: a promising new tool may be on the horizon, but decisions should be individualized, mindful of the full risk–benefit profile, and embedded within comprehensive care plans that prioritize sustainable behavior change as well as pharmacologic benefit.
- In a major randomized trial, a new oral weight-loss pill outperformed an oral semaglutide comparator on average weight loss and the proportion of participants achieving clinically meaningful thresholds.
- Improved convenience and potential adherence make oral options particularly attractive but must be balanced against unknown long-term safety and affordability concerns.
- Real-world effectiveness, long-term monitoring, and equitable access will determine whether this trial result changes standard care for obesity.
Reporting note: This article summarizes trial results and implications for clinicians, patients, and health systems. Individual treatment choices should be made with a qualified healthcare professional.