New Alzheimer’s Trigger Identified — Drug Blocks It in Early Tests
The promise of a meaningful, disease-modifying therapy for Alzheimer’s disease has been pursued for decades and resisted by complexity at every turn. Now a team of scientists reports the identification of a previously underappreciated molecular event that appears to act as a trigger for the downstream chain of processes—protein misfolding, synaptic loss, and chronic neuroinflammation—that define Alzheimer’s pathology. Equally notable: researchers describe a candidate compound that blocks that trigger in cell cultures and animal models, reversing or preventing many of the changes associated with cognitive decline. This is not a cure, and human benefit remains unproven, but the work reframes a stubborn disease in a potentially actionable way.
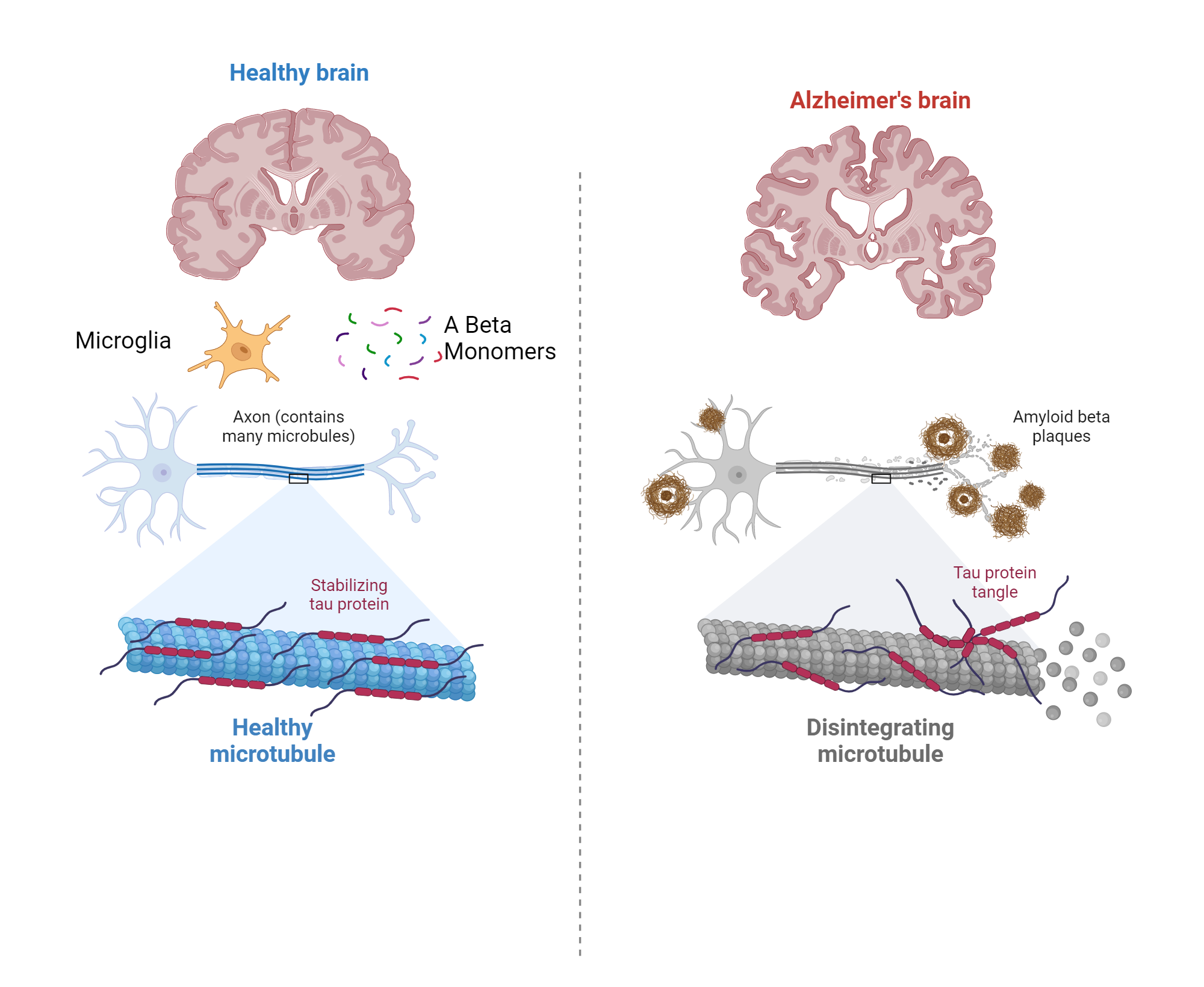
Alzheimer's disease brain pathology
Why this matters
For years Alzheimer’s research has oscillated between two core pathological hallmarks—amyloid-beta plaques and tau tangles—while the field increasingly recognizes the central role of immune and vascular factors. Identifying an upstream trigger unifies multiple strands of evidence: it offers a mechanistic road map that links molecular missteps to cellular responses and, crucially, to points where drugs can intervene. A compound that blocks the initiating event can have outsized effects downstream, reducing the need to target each pathological feature separately.
A fresh angle on a familiar foe
Alzheimer’s is not a single-pathway disease. It is better understood as a network failure influenced by aging, genetics, lifestyle, and environmental exposures. The newly described trigger is a signaling interaction that sits at the interface between stressed neurons and the brain’s innate immune cells, microglia. When neurons begin to malfunction—due to age-related changes, protein misfolding, or metabolic stress—they release a molecular cue that in turn switches microglia into a sustained pro-inflammatory, synapse-pruning state. That sustained immune activation appears to accelerate tau phosphorylation and synaptic loss, and to make amyloid deposition more toxic.
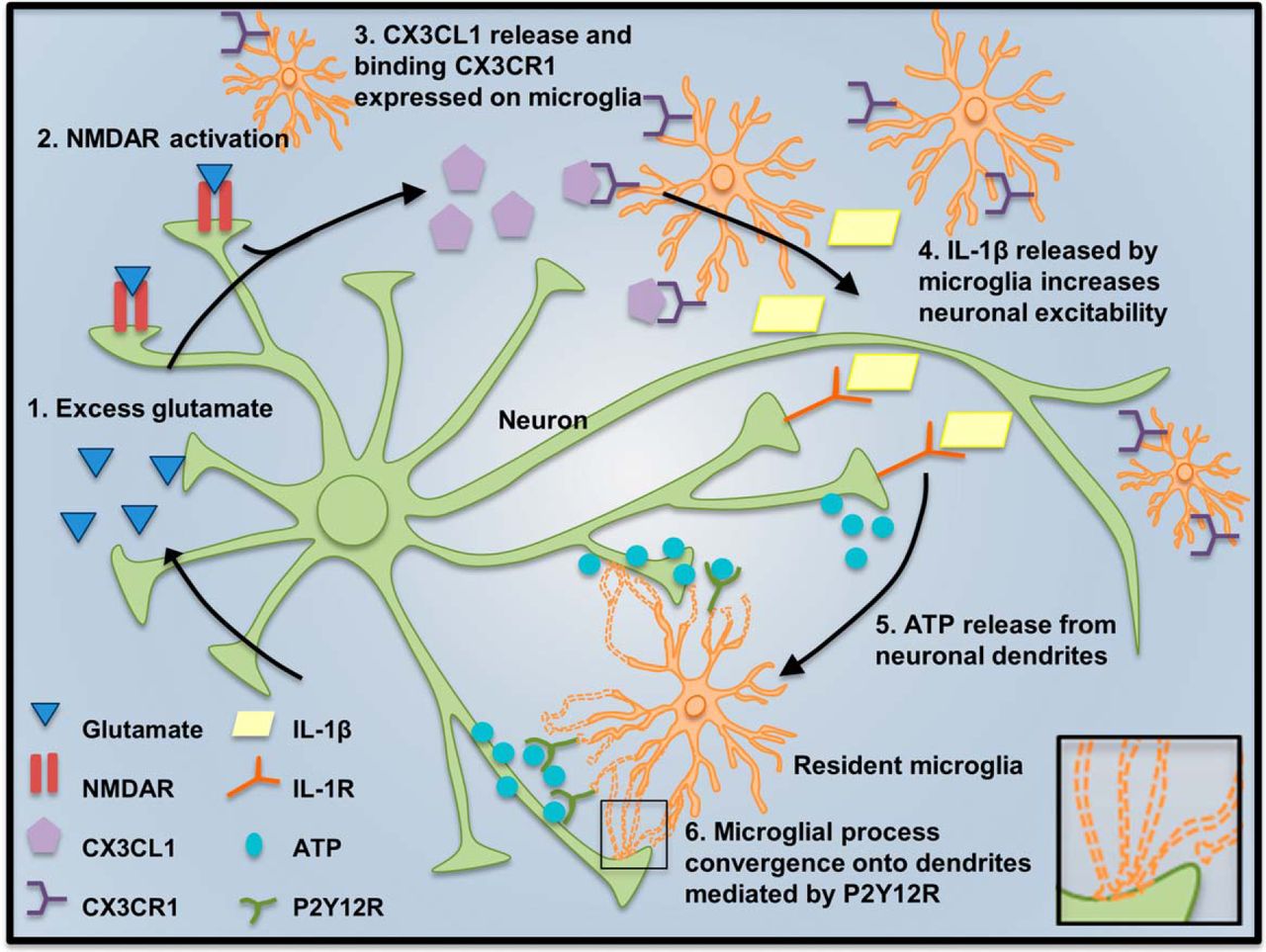
neuron microglia signaling interaction
This research reframes Alzheimer’s as an illness of maladaptive neuron–immune signaling rather than a problem isolated to amyloid or tau.
What the researchers found
The investigators used a combination of human tissue studies, cultured neurons and glia, and genetically engineered rodent models to triangulate their finding. Key observations included:
- Elevated signaling molecule — Brain tissue from individuals with early-stage Alzheimer’s showed increased levels of a signaling protein in regions vulnerable to the disease.
- Cell culture experiments — When neurons under metabolic stress released this signal, adjacent microglia shifted toward a chronic inflammatory state and increased expression of genes linked to synapse removal.
- Animal models — Mice engineered to overexpress the signaling molecule developed accelerated synapse loss, tau pathology, and measurable memory deficits compared with controls.
- Blocking the signal reverses changes — A candidate inhibitory compound administered to mice both prevented the initiation of microglial hyperactivation and, in animals with established pathology, reduced progression of synaptic loss and cognitive impairment.
preclinical drug testing mice
Each of these pieces strengthens the core narrative: the signaling interaction is not a benign byproduct of damage but a functional accelerator of disease processes.
synapse loss microscopy imaging
The candidate drug: how it works
The compound described is a small-molecule inhibitor designed to interrupt the receptor-mediated step by which neurons communicate the stress signal to microglia. Mechanistically it appears to prevent receptor clustering on microglial membranes and thereby blocks downstream activation of inflammatory gene programs and phagocytic machinery that would otherwise target synapses. In treated animals, researchers observed:
- Reduction in pro-inflammatory cytokines in brain tissue.
- Preservation of dendritic spines and synaptic markers.
- Improved performance on memory tasks compared with untreated, pathology-bearing animals.

neuroinflammation brain immune cells
Importantly, the compound was engineered to cross the blood–brain barrier at therapeutic doses and showed a tolerable safety profile in short-term toxicology studies in rodents. That said, safety in humans—and effects in human brains—are open questions.
Alzheimer's drug compound structure
Why upstream targets could change the game
Most prior therapeutic strategies have focused on clearing aggregated proteins after they have accumulated or on stabilizing downstream effects. An upstream target—if truly causal—offers several advantages:
- Multiply leverageable effects: Inhibiting a trigger can reduce multiple downstream pathologies at once.
- Earlier intervention: Targeting an initiating signal may be effective when applied in pre-symptomatic or early symptomatic stages.
- Biomarker development: A specific trigger yields measurable targets (protein levels, receptor activity) that can guide patient selection and dose-finding.
Those advantages translate into a cleaner clinical development pathway if biomarkers can robustly identify the patients most likely to benefit.
Caveats, unknowns, and hurdles
No discovery moves from bench to bedside without friction. Several unknowns loom large in this story, and any reporting about potential therapies must be measured and precise.
Translational uncertainty
Animal models approximate human disease but cannot capture its full complexity. Human brains differ in scale, life history, comorbidities, and genetic backgrounds. A signal that drives pathology in mice may have a less dominant role in humans or may act differently in the presence of common coexisting conditions such as vascular disease or diabetes.
Timing and patient selection
If the trigger is most important early in the disease cascade, the therapeutic window for maximal benefit may be before clinical symptoms emerge. That raises practical questions about screening, biomarker-based enrollment, and ethical discussions around treating asymptomatic people. On the other hand, the compound showed partial benefit in animals with established pathology—an encouraging sign that it might still be useful after symptoms begin.
Safety and long-term effects
Microglia perform essential roles—clearing infections, pruning synapses during development, and supporting neuronal health. Long-term suppression of a microglial pathway could carry risks such as impaired immune defense or unintended changes in learning and memory. Careful dose titration, intermittent dosing strategies, or selective modulators that restore homeostasis rather than bluntly block activity may be necessary.
What comes next: the path to testing in humans
Advancing from a compelling preclinical program to human trials typically follows a staged process. The immediate next steps for this candidate approach would include:
- Extended toxicology in at least two species to characterize chronic safety and identify target organ toxicities.
- Pharmacokinetic and pharmacodynamic studies to define dosing that achieves sufficient brain exposure without systemic toxicity.
- Biomarker development to measure the trigger and downstream effects in living patients—this might include blood-based assays, cerebrospinal fluid measures, or PET ligands if available.
- Phase 1 human trials focusing on safety, tolerability, and biomarker engagement in healthy volunteers and possibly in small groups of patients with early Alzheimer’s pathology.
If these steps are successful, randomized Phase 2 trials would test for signals of efficacy on cognition and function, while Phase 3 trials would be required to demonstrate a clear clinical benefit suitable for regulatory approval.
Implications for other neurodegenerative diseases
Alzheimer’s shares mechanistic themes with other neurodegenerative disorders—misfolded proteins, chronic inflammation, and synapse vulnerability. An upstream neuronal stress signal that feeds maladaptive immunity could also be relevant to Parkinson’s disease, frontotemporal dementia, and some forms of amyotrophic lateral sclerosis. If confirmed, the conceptual framework could redirect research efforts and therapeutic pipelines across multiple diseases.
- Potential to reduce multiple downstream pathologies simultaneously.
- Opportunity for early intervention guided by biomarkers.
- New mechanistic understanding could spawn multiple therapeutic approaches.
- Translational risk between animal models and humans.
- Safety concerns with long-term immune modulation.
- Need for robust biomarkers and careful patient selection.
Voices from the field
Within the scientific community, discoveries like this are greeted with cautious optimism. They open new avenues for collaboration among neuroscientists, immunologists, and clinical trialists. At the same time, experts stress the need for independent replication and transparent data sharing so that results can be validated and extended.
Early-stage discoveries are milestones—not finish lines. Reproducibility and careful clinical translation determine whether they transform patient care.
Ethical and societal considerations
Breakthroughs raise questions beyond biology. If a drug is eventually developed to prevent Alzheimer’s by blocking an upstream trigger, who will have access? How will health systems identify and screen candidates for preventive therapy? What will be the psychological impact of labeling someone as at risk based on biomarkers long before symptoms arise? These questions require policymakers, ethicists, and patient advocates to participate early in the research-to-care pipeline.
What patients and families should know
News about scientific advances often feels binary—breakthrough or bust—but the reality is incremental. For patients and families facing dementia today, the most actionable steps remain those with proven benefit: cardiovascular risk control, physical activity, cognitive engagement, sleep optimization, and management of other conditions such as diabetes and hypertension. Research advances like the one described here offer hope that future therapies may alter disease progression, but such therapies will take years of testing before they are widely available.
Conclusion: cautious optimism and a longer view
The identification of a new molecular trigger and a compound that blocks it in preclinical studies is an important development in Alzheimer’s research. It reframes the disease around maladaptive neuron–immune signaling and provides a plausible point of intervention that could influence multiple pathological pathways. Yet history counsels patience: promising preclinical findings require rigorous validation, biomarker development, and carefully phased clinical trials to determine whether they translate into safer, effective treatments for people. If this line of work fulfills its early promise, it will be because science, medicine, and society aligned—replicating results, designing thoughtful trials, and preparing systems for equitable delivery.
- An upstream neuron–microglia signaling trigger has been identified as a potential accelerator of Alzheimer’s pathology.
- A candidate brain-penetrant compound blocks this signal in preclinical models and shows promise in reducing synapse loss and cognitive deficits.
- Findings are early: human relevance, safety, biomarkers, and long-term effects must be established through careful clinical development.
This article summarizes current preclinical findings and their implications; it does not constitute medical advice.