
Humans Age in Bursts: Stanford Finds Shifts at 44 and 60
Most of us picture aging as a slow, steady slope: birthdays tick by, hair thins, knees ache, and the years accumulate in a predictable line. What if that image is wrong? What if the human body holds its breath for decades, then shifts suddenly—once in midlife and again as we approach retirement age? A recent Stanford analysis suggests just that: aging may not be entirely gradual but instead punctuated by measurable bursts of physiological change around ages 44 and 60. The idea reframes how we think about risk, prevention, and the timing of interventions intended to preserve healthspan as well as lifespan.
Stanford aging research 44 and 60
THE SURPRISING PATTERN: BURSTS, NOT A SMOOTH DECLINE
What researchers observed
The core observation is straightforward but striking: multiple physiological markers change more rapidly at two distinct life stages than they do in the decades before and after. Those changes are not tiny perturbations but patterns detectable across a variety of biomarkers—clinical measurements, molecular clocks, and functional tests—suggesting coordinated systemic shifts rather than random noise.
biological age vs chronological age
Why this matters
If aging happens in pulses, the timing of screening, prevention, and treatment matters. Intervening a few years earlier or later could miss a window when the body is most responsive to change. Insurance models, public-health guidance, and personal prevention strategies might need to be rethought to align with these inflection points.
"The body appears to flip into a different state twice: once in midlife and again near older age—moments when risk accelerates."
HOW AGING WAS MEASURED: THE TOOLS BEHIND THE FINDING
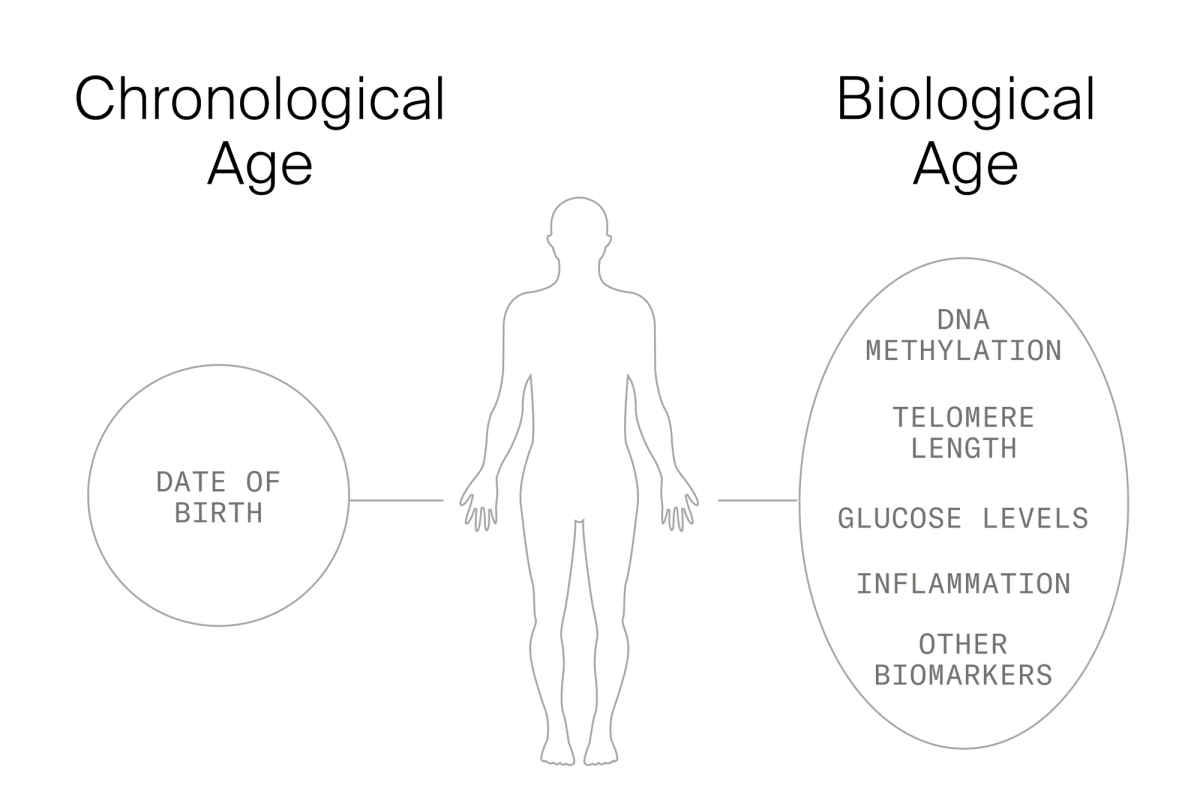
Biomarkers and biological age
Chronological age is how many birthdays you've seen. Biological age attempts to quantify how 'old' your body really is by combining information from several measurable processes. Modern approaches use: clinical biomarkers (blood pressure, glucose, inflammatory markers), molecular signatures (DNA methylation patterns known as epigenetic clocks), and functional assessments (grip strength, walking speed, cognitive screening). When multiple measures shift together, they hint at deeper organizational changes.
DNA methylation epigenetic clock
Longitudinal analysis
Detecting bursts requires following people over time rather than looking at one snapshot. Longitudinal analysis allows researchers to see acceleration or deceleration in biomarker trajectories. In this case, the researchers analyzed repeated measures across adult life and found consistent increases in the rate of change clustered around the mid-40s and around age 60.
WHY AGING MIGHT OCCUR IN BURSTS
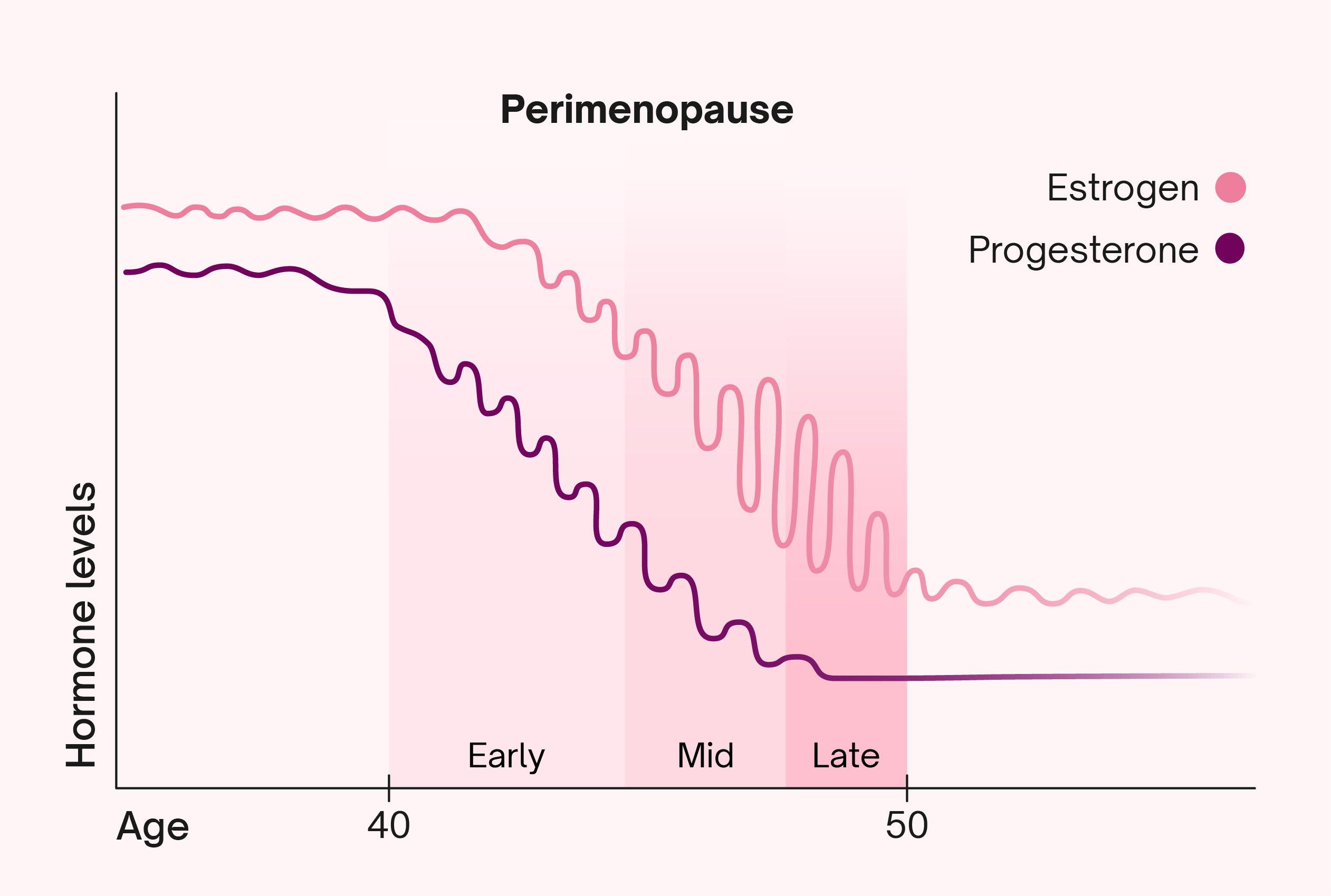
Hormonal and reproductive transitions
The mid-40s is a time when many people—particularly women—experience perimenopause, an endocrine transition that can alter metabolism, fat distribution, sleep, and cardiovascular risk. Although men do not have a sharply defined equivalent, testosterone and other hormonal axes often shift in midlife as well. Hormonal upheaval can ripple through immune function, metabolic regulation, and brain chemistry, plausibly explaining coordinated biomarker shifts.
midlife hormonal transitions perimenopause
Cumulative life stress and social change
Midlife is also a psychological and social inflection point for many: career peaks or changes, caregiving responsibilities for children and aging parents, financial stress, and lifestyle drift. Chronic stress alters cortisol regulation, inflammation, and sleep—factors that accelerate biological aging. These socioenvironmental factors often cluster with the biological transitions of midlife.
Second acceleration around 60: emerging frailty and multimorbidity
Around 60, several processes converge: cardiovascular disease risk rises, the immune system experiences immunosenescence, and cumulative damage (e.g., from years of inflammation or oxidative stress) reaches thresholds that manifest clinically. This stage often precedes more visible functional declines and an uptick in multimorbidity, which could explain a second, later burst in aging markers.
WHAT THE BURSTS LOOK LIKE ACROSS SYSTEMS
Cardiometabolic markers
Blood pressure, fasting glucose, lipid profiles, and measures of central adiposity often show pattern shifts in midlife. A modest drift in weight or waist circumference in your 30s can translate to larger metabolic consequences in the 40s, especially when paired with changes in activity or sleep.
cardiometabolic biomarkers midlife changes
Inflammation and immune function
Chronic, low-grade inflammation—often measured by C-reactive protein and other cytokines—tends to rise with age, but the rate of increase may accelerate at the identified inflection points. Simultaneous changes in immune cell composition and function are consistent with an organism-level transition toward higher vulnerability.
chronic inflammation aging markers
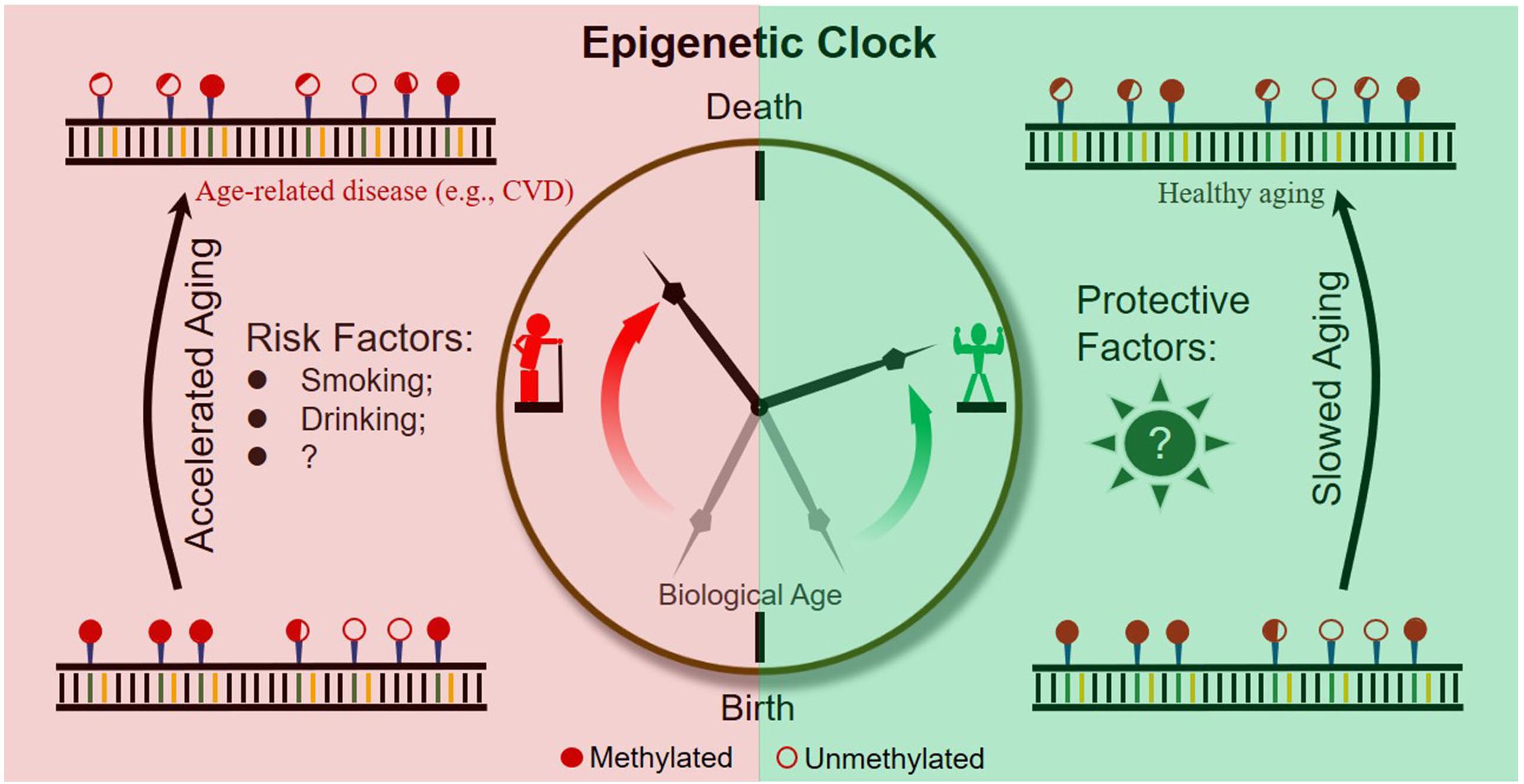
Molecular clocks and cellular markers
Epigenetic clocks derived from DNA methylation sometimes show non-linear increases tied to life events and exposures. When molecular clock acceleration aligns with clinical signals, it strengthens the case for meaningful biological transitions rather than statistical artifacts.
IMPLICATIONS FOR CLINICAL PRACTICE AND PUBLIC HEALTH
Rethinking screening timelines
Guidelines often set screening ages based on population-level risk curves calibrated to chronological age. If biological aging accelerates at midlife bursts, earlier or more frequent screening around those ages could detect risk earlier and enable interventions when they’re most effective.
Timing of interventions
Many preventive strategies—weight management, blood pressure control, statins, smoking cessation—have cumulative benefits. But if a burst represents a tipping point, starting an intervention a few years before a known inflection could blunt that transition and reduce downstream disease. Conversely, delaying until after a burst could leave missed opportunity.
PERSONAL TAKEAWAYS: WHAT YOU CAN DO NOW
Assess, don’t assume
Don’t rely solely on your calendar age as a proxy for health. Ask your clinician for periodic assessments of metabolic health, inflammation, and functional capacity. If you are approaching your mid-40s or late 50s, consider more than routine checkups—discuss targeted screening aligned with your risk profile.
Lifestyle interventions still rule
Regardless of bursts, the foundational pillars—regular physical activity, a plant-forward diet, quality sleep, stress management, and not smoking—remain the most evidence‑based ways to slow biological aging. These habits can reduce the magnitude of biomarker shifts and may delay or soften physiological bursts.
- Activity: Strength training and aerobic exercise preserve muscle mass and metabolic health.
- Nutrition: Emphasize whole foods, fiber, and moderate protein; avoid ultra‑processed foods.
- Sleep & stress: Treat sleep disorders and invest in stress reduction strategies such as mindfulness or cognitive behavioral approaches.
LIMITATIONS AND CAUTIONS
Not all studies are the same
Findings about bursts rely on the quality of the datasets and the biomarkers used. Cohort composition, measurement timing, and analytical choices can influence where and whether peaks appear. Observational findings are hypothesis‑generating rather than conclusive proof of universal life-stage cliffs.
Individual variation is large
Even if population-level bursts exist, individuals vary. Genetics, socioeconomic status, life history, and chance shape when and whether a given person experiences rapid change. Personalized assessment matters.
Avoid deterministic thinking
Discovering a population inflection doesn't mean every person will follow it. It also doesn't doom someone to rapid decline once they hit a particular birthday. The presence of a burst indicates risk concentration, not inevitability.
RESEARCH NEXT STEPS
Mechanistic studies
The next phase is to dig into causes: endocrine signaling, immune remodeling, cumulative damage pathways, and psychosocial stressors. Animal models and mechanistic human studies can test whether altering a candidate pathway changes the timing or magnitude of bursts.
Intervention timing trials
Randomized trials that start preventive measures at different ages could test whether timing around detected inflection points yields larger benefits. Trials that monitor molecular clocks as secondary outcomes would help bridge clinical and cellular perspectives.
Population equity
Researchers should ask whether burst timing differs by race, gender, occupation, or socioeconomic status. If social adversity shifts or amplifies bursts, targeted public-health interventions could reduce disparities in later-life disease.
CONCLUSION: A NEW WAY TO THINK ABOUT AGING TIMELINES
The thought-provoking notion that aging advances in bursts rather than by a steady slope reframes prevention and prioritization. If validated and refined, the pattern suggests midlife and the decade before typical retirement are especially consequential for shaping later-life health. Clinicians, policymakers, and individuals may all benefit from shifting attention to those windows—assessing risk, intensifying prevention, and designing trials that test timing as much as the intervention itself.
- A Stanford analysis found population-level acceleration in biological aging around ages 44 and 60, implying non-linear aging trajectories.
- Bursts could be driven by endocrine transitions, cumulative stress, and rising multimorbidity; they raise the importance of timing for screening and prevention.
- Foundational lifestyle measures—exercise, nutrition, sleep, and stress reduction—remain essential and may blunt the impact of these transitions.
- Further research should test mechanisms, evaluate equity, and run trials that consider the timing of interventions.
Final thought
We still celebrate birthdays one by one, but biology may not. Paying attention to the moments when our bodies are most likely to change could be the difference between adding years to life and adding life to years.