How Ozempic and Wegovy Mistakes Sent Thousands to Poison Control
The recent boom in semaglutide-based medications — branded most commonly as Ozempic for diabetes and Wegovy for chronic weight management — has been a pharmaceutical success story and a public-health puzzle at the same time. Alongside dramatic demand and media attention, poison-control centers, emergency departments, and pediatricians have reported a marked increase in accidental exposures, medication mix-ups, and misuse. Patients and families find themselves navigating new devices, unfamiliar dosing, and bright social-media-driven narratives about rapid weight loss. The result: thousands of anxious calls, some preventable, many revealing weaknesses in how modern medicines reach and are used by everyday people.

Ozempic injector pen
The surge: what happened and why it matters
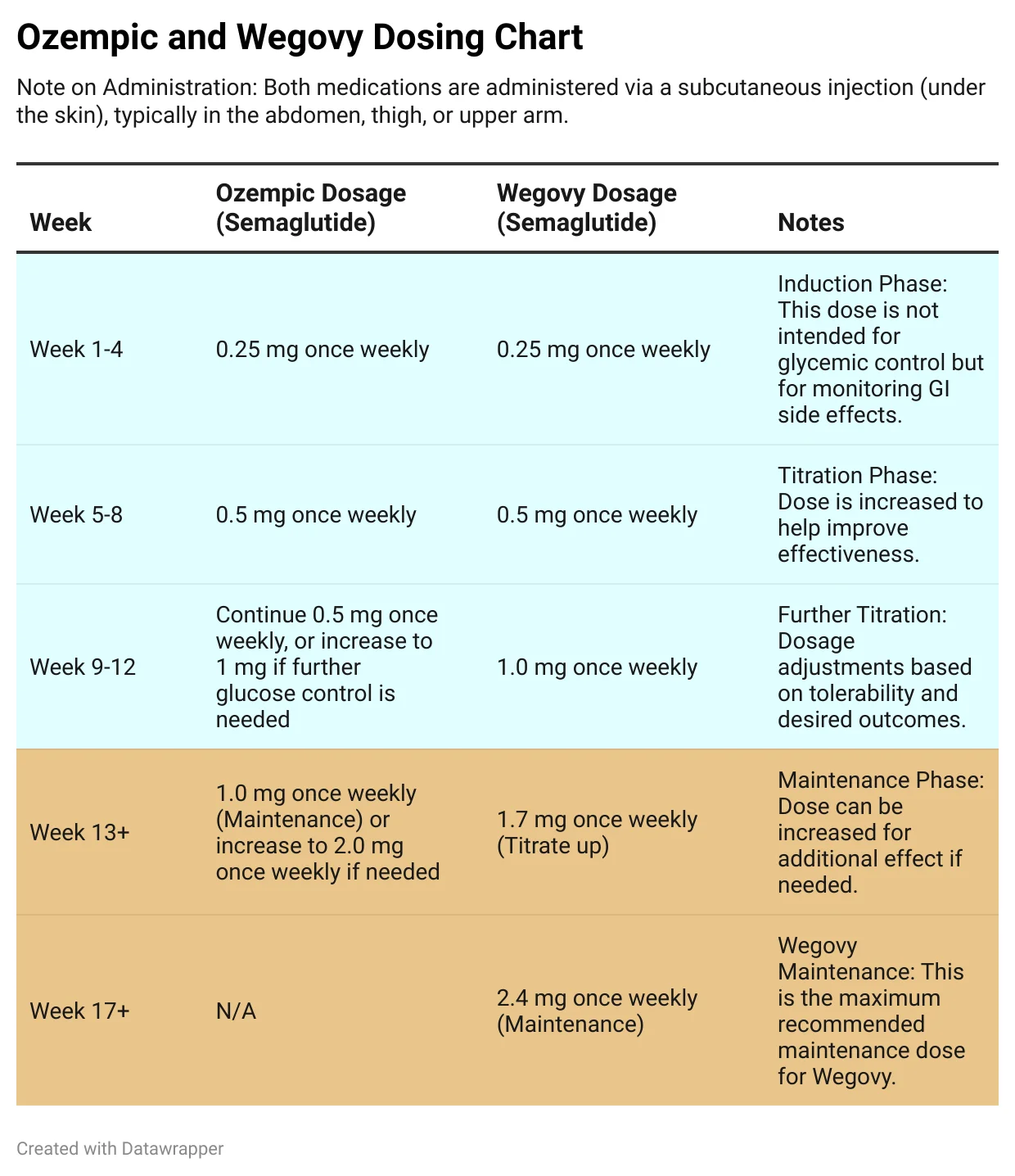
When a medicine moves from niche to mainstream, the velocity of change matters as much as the drug itself. Semaglutide arrived as a prescription medication for type 2 diabetes, then was approved at a higher dose for chronic weight management. That wider approval, a stream of celebrity endorsements, and social-media amplification turned injectable therapy into an in-demand commodity almost overnight. Pharmacies, clinics, and prescribers scrambled to keep up, and patients — eager for outcomes — sometimes stretched instructions or experimented with dosing schedules they saw online.
In parallel, shortages and distribution strains created environments where sharing, repackaging, or improvisation felt like pragmatic choices. Sharing an extra pen with a friend, transferring solution between syringes, or misreading a label are easy steps on a short chain that ends with an accidental exposure or a call to poison control.
A medication’s safety is only as strong as the systems that deliver it — from manufacturer labeling to the moment it’s stored in a kitchen cabinet.
How semaglutide drugs work — and why that matters for safety
Semaglutide belongs to a class of drugs called GLP-1 receptor agonists. They mimic a hormone that helps regulate appetite, gastric emptying, and insulin release. For people with diabetes, that translated into improved blood-sugar control. For people with obesity, higher doses delivered sustained weight loss by reducing appetite and slowing digestion.

GLP-1 receptor agonists
That beneficial effect is also why accidental exposure can create symptoms that concern caretakers and clinicians: sudden nausea, vomiting, low blood sugar (hypoglycemia), dizziness, and, in small children especially, pronounced lethargy or inability to keep fluids down. Recognizing a drug’s mechanism helps clinicians triage exposures: symptoms are predictable and often treatable, but timing and dose matter.
Where the chain breaks: common causes of accidental exposure
The cascade that leads to a poison-control call typically involves multiple small failures. Fixing any one of them reduces overall risk.
Packaging and device confusion
Many semaglutide products are delivered in prefilled injector pens or multi-dose vials with small labels, similar-looking boxes, and dosing scales that differ by brand. Patients used to oral pills can be confused by pen clicks, removable caps, and dose-selection dials. A child left unsupervised with a pen, or a caregiver who mistakes the device for an insulin pen, can lead to incorrect administration. Pharmacy repackaging during shortages — moving drugs into different containers or writing labels by hand — increases the chance of misidentification.
Wegovy medication packaging
Sharing, hoarding, and informal distribution
Social pressures and supply constraints have produced behavior rarely discussed in medical journals: sharing prescriptions. Whether to save money, help a friend, or because a scheduled appointment was missed, people sometimes give or receive someone else’s medication. That practice bypasses counseling from a prescriber or pharmacist and obliterates dosing safeguards.
Off-label dosing and DIY attempts
Another driver is online communities experimenting with fractionated doses, alternating schedules, or repurposing syringes. Well-intentioned experimentation can become dangerous when people attempt to split pens, draw from vials without proper sterile technique, or use dosing scales not intended for semaglutide formulations.

Semaglutide vials syringes
Pediatric vulnerabilities
Children are uniquely at risk in household medicine exposures. A drop or a lick from a pen, a cap left on a low coffee table, or an unlocked bag with multiple devices can expose a toddler to a dose that, relative to body size, is huge. Pediatric physiology magnifies some adverse effects: dehydration from vomiting and reduced intake can escalate quickly. Poison-control professionals stress that even small quantities require prompt evaluation.
Pharmacy and prescribing errors
Pharmacies under pressure can make dispensing errors — wrong product, wrong concentration, or mislabeling. Prescribers who are inexperienced with injectables may not provide enough counseling on storage or device use. Electronic prescribing systems that auto-fill incorrect quantities or select the wrong formulation play a role too. These are systems problems, not individual blame, but they translate into misplaced injections and urgent calls.
Clinical consequences: what poison control and ERs are seeing
Most exposures reported to poison-control centers result in phone triage and home management advice. But emergency departments have seen cases that required monitoring, intravenous fluids, antiemetics, and blood-sugar checks. For adults, severe hypoglycemia is the most feared complication. For children, persistent vomiting, lethargy, or respiratory compromise can prompt observation and supportive care.
Poison control center
Clinicians prioritize stabilizing airway, breathing, and circulation; correcting hypoglycemia; and treating dehydration. Because semaglutide slows stomach emptying, anti-nausea medications and attentive fluid management are common interventions. Importantly, there is no simple antidote for GLP-1 agonists, so care is supportive rather than curative.
Supportive care — fluids, nausea control, and careful blood-sugar monitoring — is the backbone of treatment for accidental semaglutide exposure.
What patients and families should do right now
Actions that reduce risk are practical and mostly low-cost. The most important step is conversation: prescribers must explain, and patients must ask, about storage, device appearance, and what to do if someone else uses the medicine.
- Store medications out of reach and sight — high cabinets or locked boxes are simple and effective.
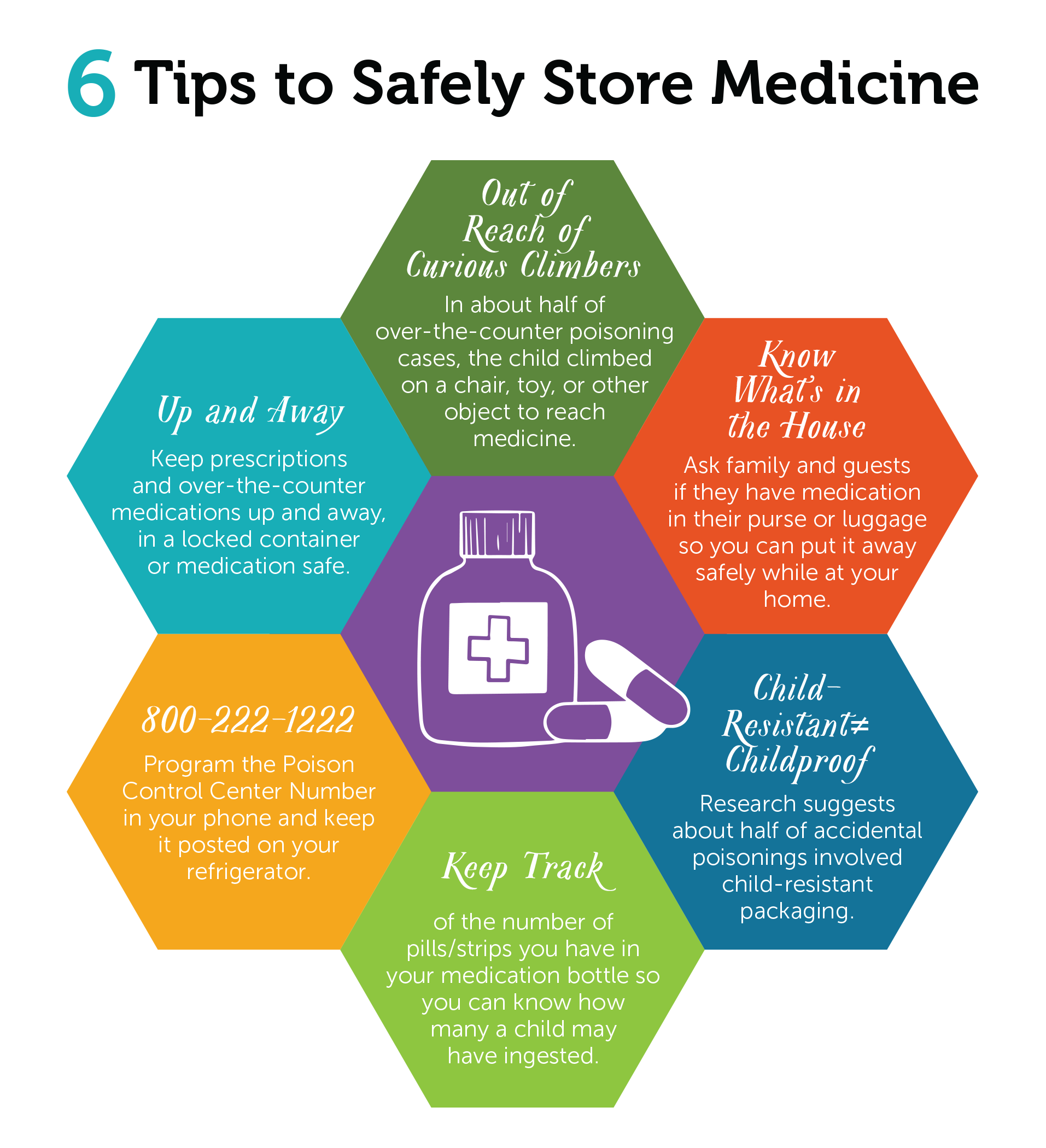
Medication storage safety
- Keep devices in their original packaging with manufacturer labels intact; avoid decanting into other containers.
- Never share prescription medications — even with family or friends. Dosing is individualized and sharing bypasses professional guidance.
- If an exposure occurs, call your local poison-control center immediately — they provide free, expert advice and can tell you whether an ER visit is needed.
- Bring the device or packaging to any medical visit so clinicians can see exactly what was involved and advise appropriately.
What pharmacies, prescribers, and manufacturers can change
Preventing these incidents requires multi-layered solutions: clearer labeling, better patient education, and systems that reduce cognitive load on clinicians and patients alike.
Design and labeling improvements
Manufacturers can standardize clearer, high-contrast labels that distinguish concentrations and intended indications. Distinctive color coding for diabetes versus weight-loss formulations, tamper-evident packaging, and single-use safety caps could reduce mistaken identity. Design changes that make pens visibly different from insulin devices would directly address one common confusion.
Pharmacy workflow and counseling
Pharmacies should prioritize face-to-face counseling at the point of dispensation for any injectable. When workload spikes, an explicit brief checklist that includes showing the pen, demonstrating dose selection, and confirming storage can prevent errors. Pharmacist-led training for nursing homes and caregivers can reduce downstream exposures in communal settings.
Prescriber responsibility and shared decision-making
Clinicians should document that device education occurred, use teach-back methods, and discuss risks of sharing or repurposing medication. For patients with young children or cognitive impairment at home, discussing locked storage or alternative therapies may be appropriate. Counseling should include concrete examples — not just abstract warnings — to make the risk tangible.
Policy and regulation: opportunities and tensions
Regulators face a delicate balance: making products accessible while ensuring public safety. Policies that clarify labeling requirements, enforce child-resistant packaging, and support post-marketing surveillance can make a measurable difference. At the same time, overburdensome rules could worsen shortages or limit patient access. The right approach is targeted regulation informed by real-world incident data, not broad restrictions that ignore nuance.
Communication in the age of social media
One modern twist is the speed at which anecdote becomes prescription in online communities. Viral posts about dramatic weight loss drive demand; videos showing injections without context normalize risky behavior. Public-health messaging must meet people where they are: clear, shareable short-form content about safe handling, the dangers of sharing, and when to call poison control can blunt misinformation’s reach.
Stories from the frontline
Emergency nurses describe late-night phone calls from frantic parents who found a pen on the floor. Pharmacists recount patients who brought in empty boxes and asked for advice after a roommate used their supply. Poison-center specialists recall the pattern: an initial swell of uncertainty, followed by practical guidance and relief — but also cases where delayed recognition led to hours of worsening symptoms. These anecdotes underline a truth: the same drugs that offer clinical benefit can cause real harm when the safety net frays.
People don’t set out to create emergencies; they often lack clear instructions, time, or a safe place to store medication.
Practical protocols for clinicians and institutions
Hospitals and clinics can adopt standardized protocols to prevent exposures: mandatory device education for first-time users, checklists for dispensing, and routine home-safety screening questions — for example, asking whether children live in the home or if the patient tends to share medications. Nursing homes and assisted-living facilities should include semaglutide pens in their medication reconciliation and storage audits.
What to expect when you call poison control
When you call, specialists will ask what substance, how much, when it happened, and who was exposed. They’ll want to know the person’s age, weight, symptoms, and any preexisting conditions. Often, they recommend monitoring at home with clear return precautions; sometimes they advise immediate ER evaluation. Keep the packaging handy — it speeds accurate advice.
- Effective treatment for diabetes and obesity when used correctly.
- Long-lasting dosing with weekly injections for many patients.
- High risk of adverse effects if misused or accidentally ingested.
- Device confusion and social-media–driven sharing increase exposure risk.
Final perspective and actionable takeaways
The rapid uptake of Ozempic, Wegovy, and other semaglutide products has delivered demonstrable benefits for many patients. But success without systems creates hazards. Thousands of poison-control calls are not an indictment of the medicines themselves; they are a signal about the fragile interface between a complex drug and everyday life.
- Store injectables securely and keep original packaging to avoid confusion.
- Never share prescription medications — dosing and indications are individualized.
- Pharmacies and prescribers must provide hands-on device education and use teach-back techniques.
- Call poison control immediately after any suspected exposure; they often prevent unnecessary ER visits.
- Regulatory and industry changes to labeling and packaging can meaningfully reduce accidental exposures.
Conclusion
Modern therapeutics work best when paired with modern safety systems. The surge of semaglutide use has exposed weak links in distribution, communication, and household storage practices. Addressing those weak links — with better design, clearer counseling, and smarter public messaging — will reduce accidental exposures and restore trust. For patients, caregivers, and clinicians, the most immediate win is simple: talk, demonstrate, and secure. Those three actions will keep the medicines where they belong — helping people, not sending them to the phone line for emergency help.
If you suspect accidental exposure to a medication, contact your local poison-control center or emergency services immediately.