Creatine for Depression: Emerging Evidence and Guidance
The idea that a supplement widely used by athletes could also ease the heavy fog of depression feels at once hopeful and improbable. Yet over the past decade scientists have been investigating creatine — the same molecule familiar to gym-goers for boosting muscle energy — as a possible adjunct to conventional treatments for major depressive disorder. This feature walks through the science, the trials, the risks, and the practical questions patients and clinicians are asking: What does the evidence actually show? How might creatine work in the brain? Who might benefit, and how should it be taken if considered?
depression mood disorder
Why researchers are interested in creatine
A different angle on depression
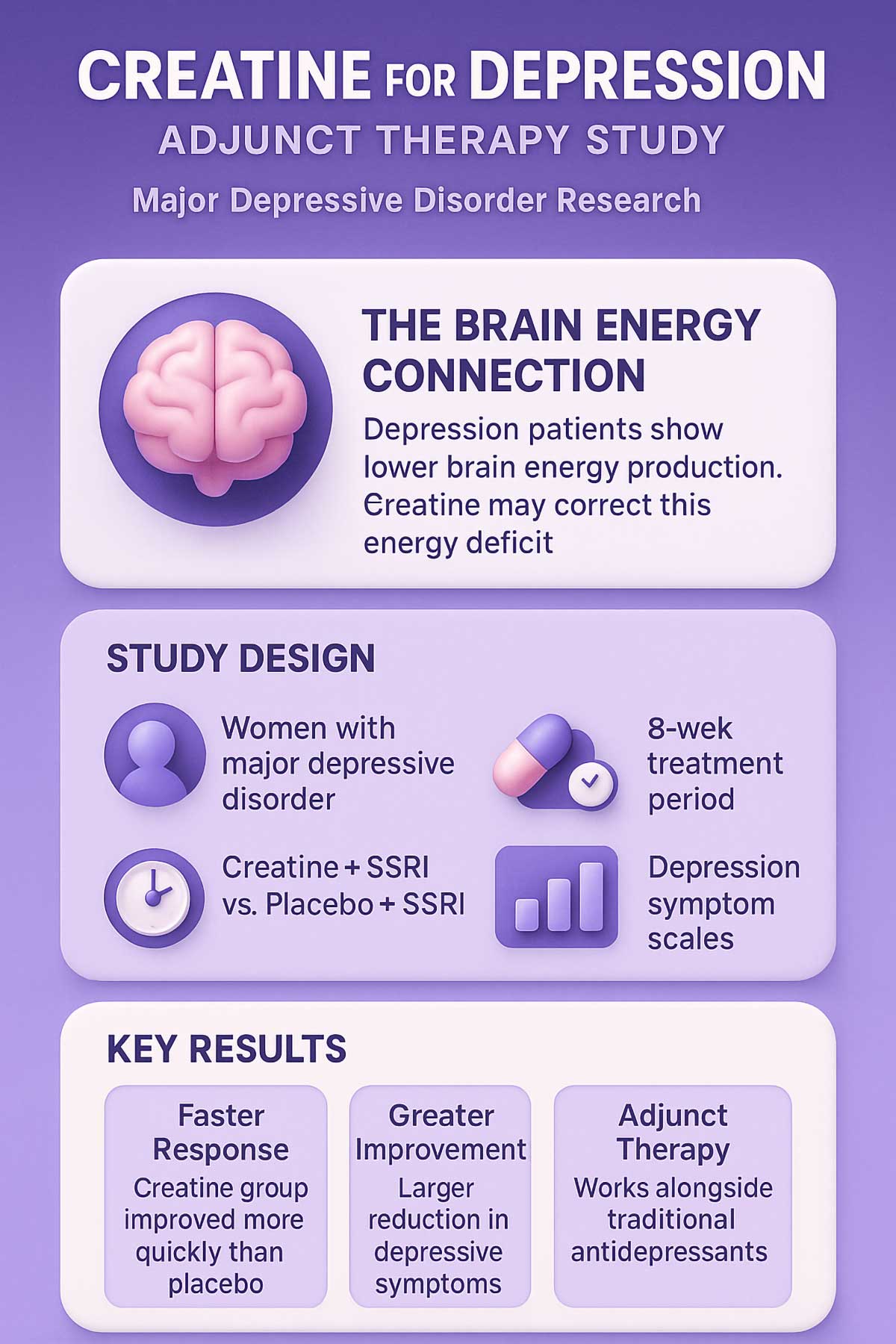
For decades, the mainstream view of depression focused heavily on neurotransmitters such as serotonin and norepinephrine. More recently, researchers have widened the lens to include brain energy metabolism, inflammation, synaptic plasticity, and mitochondrial health. Creatine sits at the intersection of those interests because its central biological role is to store and shuttle energy in cells by buffering adenosine triphosphate (ATP).
Creatine is found throughout the body but concentrated in high-energy tissues — skeletal muscle, heart, and brain. In neurons, creatine and its phosphorylated form (phosphocreatine) help maintain rapid energy supply during synaptic activity. That function has drawn attention because depressive disorders are associated in many studies with altered brain metabolism, reduced synaptic connectivity, and, in some cases, signs of mitochondrial dysfunction.
From bench to bedside
Preclinical experiments show creatine can affect brain cells in ways relevant to mood: it supports ATP availability, influences cellular calcium handling, modulates glutamate and GABA signaling indirectly, and can blunt inflammatory pathways. Those biological plausibility signals prompted small clinical trials and pilot studies testing whether oral creatine supplementation could improve depressive symptoms — either alone in preliminary studies or, more commonly, as an adjunct to antidepressant medications.
Creatine's appeal is simple: it's inexpensive, widely available, and—if safe—could offer a novel, metabolism-focused addition to mental health care.
How creatine works in the brain
Energy buffering and synaptic resilience
At its core, creatine provides a rapid reserve of high-energy phosphate bonds that neurons tap into when demand spikes. By stabilizing ATP levels, creatine may help sustain the energetically expensive processes involved in neurotransmission, plasticity, and cellular repair. These effects could translate into better synaptic functioning and resilience under stress — mechanisms closely tied to mood regulation.
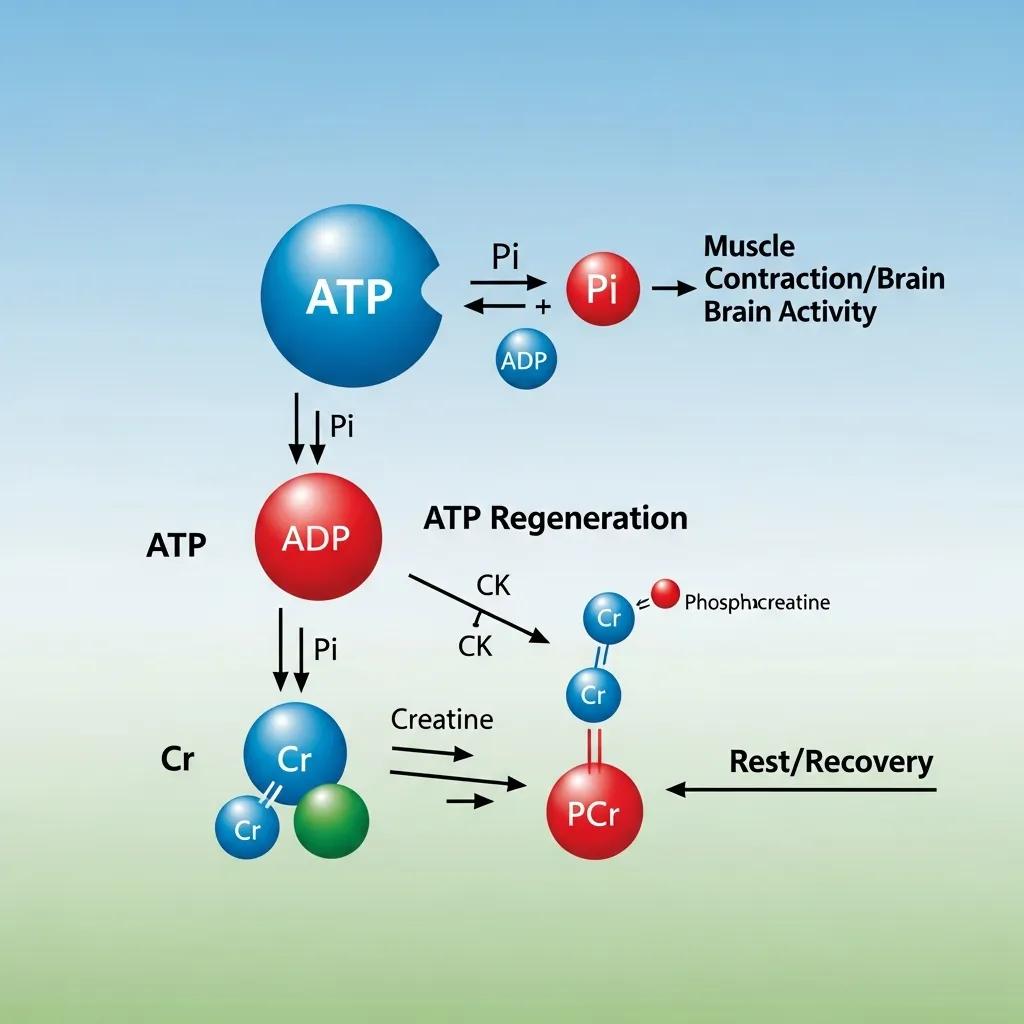
brain energy metabolism ATP
Neurochemical and neuroprotective effects
Beyond energy, creatine appears to influence neurochemical systems and neuroinflammation. Animal studies indicate it can modulate glutamatergic signaling and reduce markers of oxidative stress and inflammation, both of which are implicated in depressive states. Creatine also supports mitochondrial integrity, and because mitochondrial dysfunction has been observed in some people with depression, the supplement’s protective effects at that level are particularly intriguing.
What the clinical evidence shows
Types of studies conducted
The human evidence is still emerging and should be regarded as preliminary. Researchers have carried out a mix of study types: small randomized controlled trials, open‑label studies, and pilot investigations. Most trials have examined creatine as an adjunct — added to standard antidepressant therapy — rather than as a standalone replacement for treatment. Results are mixed but promising in specific contexts.
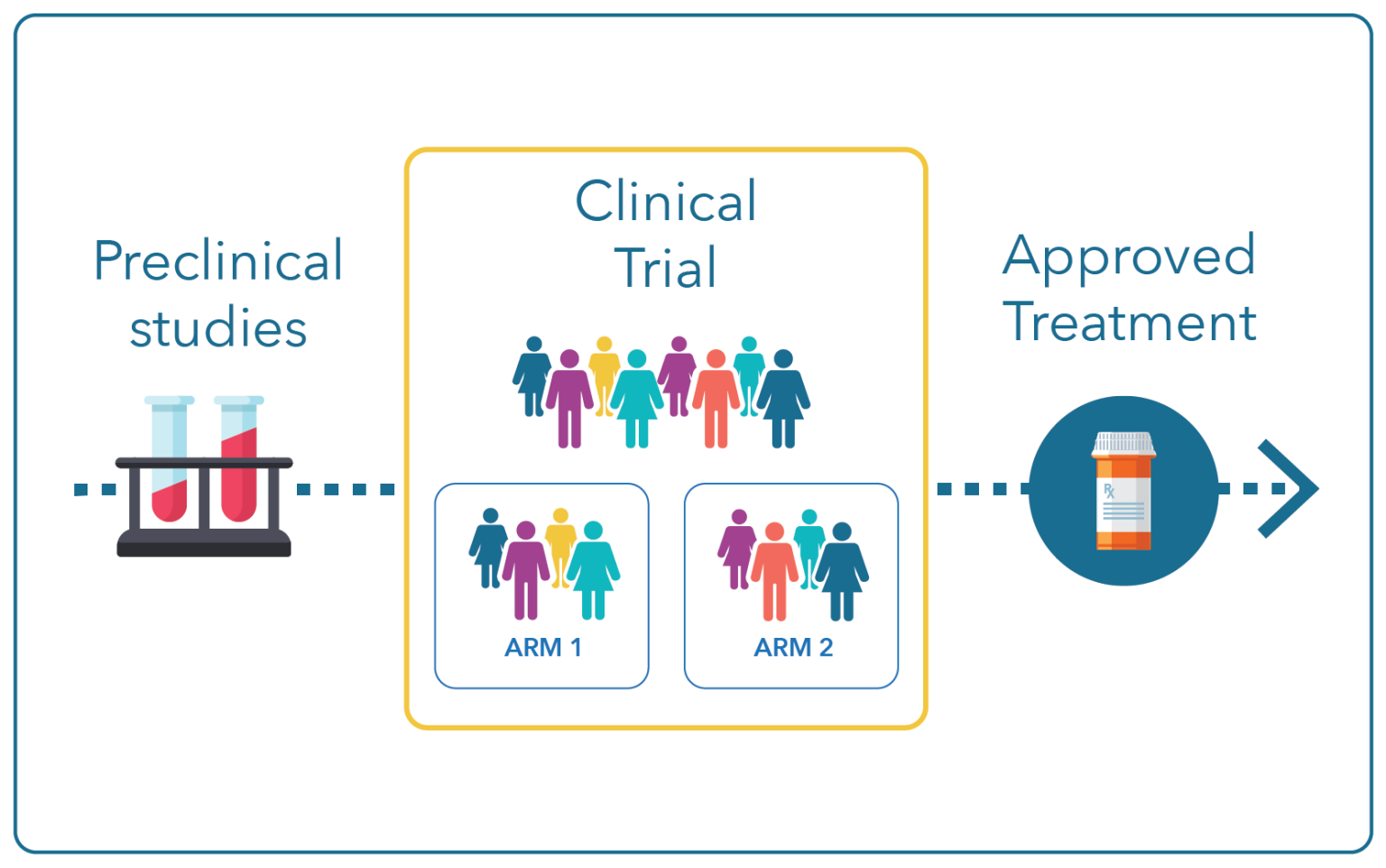
clinical trial research study
Patterns in the findings
Across studies there are a few consistent themes: some trials report faster or greater improvement in depressive symptoms when creatine is added to antidepressants, especially in certain subgroups; effect sizes vary and not every study is positive; sample sizes are generally small; and follow-up periods are limited. Because of this heterogeneity, mainstream clinical guidelines have not broadly adopted creatine for depression, but individual clinicians and researchers view it as a candidate for further, larger trials.
Who might benefit — and who should be cautious
Potential beneficiaries
Evidence hints that creatine augmentation may be most useful as an add-on for people already taking antidepressants who have partial or delayed response — in other words, those who have some benefit but remain symptomatic. Some studies have suggested sex differences in response, with signals stronger in women in limited datasets, though the reasons for this are not yet clear and require confirmation.
Groups needing caution
People with pre-existing kidney disease are usually advised to avoid or be closely monitored with creatine because of theoretical risks to renal function and because most safety data come from healthy adults. Pregnant or breastfeeding people and children or adolescents should not begin supplements without specialist advice, as long-term safety data for these groups in the context of mood disorders are lacking.
Dosing, form, and practical use
What formulations were studied
Most human trials used creatine monohydrate, the most common and least expensive form. That makes the research findings more directly transferable to over-the-counter products, provided the supplement is pharmaceutical‑grade and properly labeled.

creatine monohydrate powder

creatine supplement capsules
Typical dosing strategies
Common regimens outside psychiatric care follow sports nutrition patterns: a short loading phase (for example, roughly 20 grams per day divided across doses for 5–7 days) followed by a maintenance dose (often 3–5 grams daily). Clinical trials exploring mood effects have used both loading and maintenance and sometimes only maintenance dosing; protocols vary. A conservative, well‑tolerated approach many clinicians suggest if they agree to try supplementation is 3–5 grams per day of creatine monohydrate.
Safety and side effects
Common, mild effects
Creatine is generally well tolerated. The most frequently reported effects are modest weight gain due to water retention in muscle and occasional stomach upset when large doses are taken at once. These effects are usually reversible when supplementation stops.
Serious concerns and monitoring
Serious adverse outcomes in healthy adults are uncommon in the research record, but because supplements are less tightly regulated than prescription medicines, quality control matters. People with impaired renal function should avoid starting creatine without evaluation because creatinine — a marker commonly used to monitor kidney health — is derived from creatine metabolism and can be harder to interpret. When clinicians consider creatine, they may baseline serum creatinine and renal function and then repeat testing if clinically indicated.
kidney function blood test
Interactions with psychiatric medications
There is no well-established drug interaction that prohibits creatine use with standard antidepressants. Most research investigated creatine as an adjunct to selective serotonin reuptake inhibitors and other commonly prescribed antidepressants without detecting clear negative interactions. Still, any change in supplement or medication regimen should be coordinated with the treating clinician, who can monitor response and tolerability.
Practical guidance for patients and clinicians
How patients can approach the idea
If you're considering creatine to help depressive symptoms: 1) discuss it with your prescribing clinician rather than starting it on your own; 2) be clear that current evidence is preliminary and augmentation, not replacement, of established treatments; 3) ask about baseline kidney tests if you have relevant medical history; 4) set realistic expectations — it is not a guaranteed fix and tends to be studied as an add-on.
How clinicians might incorporate creatine
Clinicians curious about creatine should weigh the evidence case-by-case. For patients with partial response to antidepressant therapy who have no contraindication, a trial of creatine monohydrate at 3–5 g/day with monitoring could be reasonable within shared decision-making. Document baseline symptom severity, obtain relevant labs if indicated, and set a review point to assess benefit and side effects.
Research gaps and next steps
Key questions remain. Larger randomized controlled trials with diverse populations and longer follow-up are needed to confirm efficacy, define which subgroups benefit most, and clarify optimal dosing. Researchers are also interested in biomarkers that could predict response — for example, baseline measures of brain energy metabolism or inflammation — and in whether creatine’s effects extend to other psychiatric conditions or cognitive symptoms related to depression.
Conclusion: a cautious, hopeful perspective
Creatine is an intriguing candidate in the search for new, affordable tools to help people with depression, especially where traditional treatments produce incomplete relief. The biological rationale is strong, and early clinical signals are promising, but evidence is not yet definitive. For motivated patients with appropriate medical clearance, a carefully monitored trial of creatine monohydrate as an adjunct to prescribed therapy may be reasonable. It is not a replacement for evidence-based psychotherapy or medications when those are indicated.
- Creatine supports brain energy metabolism and has biological plausibility for benefit in depression.
- Clinical evidence is preliminary but suggests possible benefit when used as an adjunct to antidepressants in some people.
- Typical practical dosing is 3–5 g/day of creatine monohydrate; safety monitoring is advised for those with kidney issues.
- Discuss supplementation with your clinician and use it only as part of a comprehensive treatment plan.
This article summarizes emerging research and general guidance; it is not medical advice. Consult a healthcare professional before starting any supplement regimen.