
Cold Sores and Babies: The Hidden Risk of HSV Encephalitis
The image most people have of a cold sore is a minor nuisance: a tingle, a blister at the lip, a tube of ointment in the drawer. But for newborns, that familiar lesion can be a conduit to catastrophe. This article follows the outline of a single, heart-rending case—an otherwise healthy infant who developed herpes simplex virus (HSV) encephalitis after exposure to an adult with a cold sore—and uses it to explore how HSV behaves in newborns, how clinicians diagnose and treat HSV encephalitis, and what parents, relatives, and healthcare workers can do to prevent similar tragedies.
“What seemed like a harmless kiss became the beginning of a medical emergency.”
A Baby’s Story
The baby was born full-term, took to feeding well, and went home within 48 hours. Family celebrated the arrival; visitors flowed through the door. A beloved aunt—who had suffered occasional cold sores for years—held the infant several times and kissed the baby on the cheek and lips. Two weeks later the child developed a fever and was irritable. Within 48 hours the infant had a seizure and was brought to an emergency department. Blood tests, a lumbar puncture, and brain imaging ultimately led clinicians to diagnose HSV encephalitis. Antiviral therapy was started, but the infant required intensive care. The course that followed included prolonged antiviral treatment, monitoring for neurologic damage, and a long road of follow-up therapies and developmental surveillance. The family was left with guilt, grief, and a question asked by many parents: how could a cold sore do this?
A newborn presenting with fever and seizures—a critical sign of possible HSV encephalitis
What Is Herpes Simplex Virus (HSV)?
A brief definition

A typical cold sore on the lip—the familiar HSV-1 lesion that can pose serious risks to newborns
How the virus behaves
HSV infects epithelial cells at the site of contact, then travels along nerves to establish latency in nerve ganglia. During reactivation, the virus replicates and is shed at mucocutaneous sites—often before a lesion is visible. That means viral shedding (and risk of transmission) can happen during that tingling prodrome or even with seemingly healed skin. In adults with normal immune systems, outbreaks are usually localized and self-limited. In newborns, however, the immature immune response and the routes of exposure make HSV a far more dangerous pathogen.
How Cold Sores Can Put Infants at Risk
There are three main ways that HSV threatens newborns:
- Perinatal transmission: Exposure during delivery, particularly if a mother has active genital HSV, can infect the baby as it passes through the birth canal.
- Postnatal transmission: After discharge, caregivers or visitors with oral or genital HSV can transmit the virus through direct contact—kissing the face, hands, or feeding implements; touching a lesion and then the baby’s skin; or inadequate hand hygiene.
- In utero transmission: Rare, but possible, when maternal virus crosses the placenta.
In the case described above, postnatal transmission from a visitor with a cold sore is the most likely scenario. Importantly, adults often underestimate how contagious they may be when they have an active lesion—or during the prodrome when no blister has formed.
Recognizing HSV Encephalitis in Infants
Early signs and symptoms
HSV infection in newborns has a spectrum of presentations. Clinicians classify neonatal HSV into three broad patterns: localized skin/eye/mouth disease; disseminated disease affecting multiple organs (including liver, lungs, and blood); and central nervous system (CNS) disease—HSV encephalitis. Signs that should raise immediate concern include:
- Fever—often the first sign, but sometimes absent in very young infants.
- Feeding difficulties or poor latch.
- Irritability, lethargy, or unusual high-pitched crying.
- Seizures—a red flag for CNS involvement.
- Focal neurologic signs such as decreased responsiveness, abnormal movements, or poor muscle tone.
- Skin lesions—tiny grouped vesicles or scabbed sores, though these may be absent in pure CNS disease.
Because initial symptoms are nonspecific and overlap with many common neonatal problems, the window to act can be narrow; any concerning neurologic sign in a young infant requires urgent evaluation.
Diagnosis: How Doctors Confirm HSV Encephalitis
Key diagnostic steps
When HSV encephalitis is suspected, clinicians typically pursue:
- Lumbar puncture (CSF analysis) to look for inflammatory changes and to run polymerase chain reaction (PCR) testing for HSV DNA—PCR is highly sensitive and specific and is the gold standard for diagnosing HSV in the CNS.
- Blood tests including PCR and liver function tests, because disseminated HSV can damage the liver.
- Neuroimaging—MRI is preferred for identifying the areas of brain inflammation typical of HSV encephalitis, often affecting temporal lobes, though findings vary in neonates.
- Electroencephalogram (EEG) if seizures occur or to assess encephalopathy.
Time matters. Because delay in antiviral therapy is strongly associated with worse outcomes, empiric treatment with intravenous acyclovir is started when suspicion is high—even before confirmatory PCR results return.
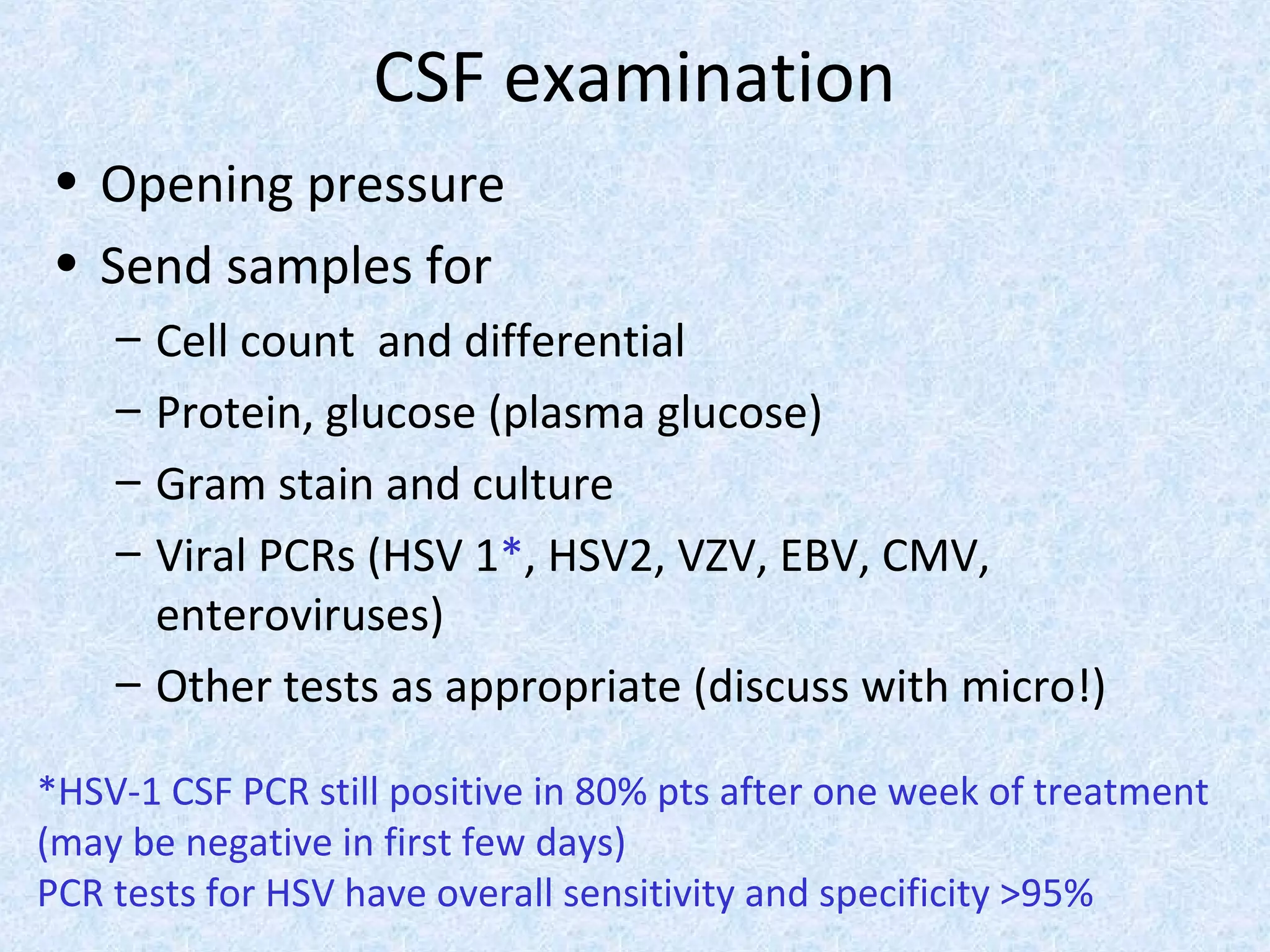
PCR testing of cerebrospinal fluid—the gold standard diagnostic test for HSV encephalitis in newborns
Treatment and prognosis
Antiviral therapy
Acyclovir is the cornerstone of therapy for neonatal HSV and HSV encephalitis. Higher doses and intravenous formulation are used in newborns with suspected or confirmed CNS disease. Treatment is prolonged—often a minimum of 14 to 21 days for CNS involvement, followed in some cases by oral suppressive therapy, depending on clinical course and specialist recommendations.
Intravenous acyclovir—the cornerstone medication for treating neonatal HSV encephalitis
Supportive care and complications
Beyond antiviral therapy, infants may require ventilatory support, management of seizures, and care for complications such as liver dysfunction or disseminated infection. Despite treatment, HSV encephalitis can cause long-term neurologic sequelae—developmental delay, motor deficits, hearing impairment, or epilepsy. Early treatment improves outcomes, but prevention remains the most powerful tool.

A neonate receiving intensive care with IV therapy for HSV encephalitis
Prevention: Practical Steps Families and Caregivers Can Take
Common-sense precautions
Preventing postnatal HSV exposure requires awareness and simple behavioral changes:
- No kissing newborns on or near the mouth—especially by anyone with a current cold sore or a recent history of one.
- Hands matter: rigorous handwashing before contact with the baby, after changing diapers, and after touching one’s face.
- Visitors with symptoms should stay away—reschedule visits if someone has a sore throat, fever, blister, or prodromal tingle.
- Avoid sharing items that touch the baby’s mouth—utensils, pacifiers, or cups—with anyone who has an active lesion.
Rigorous handwashing is essential before any contact with a newborn

Refraining from kissing newborns on the face is a critical preventive measure
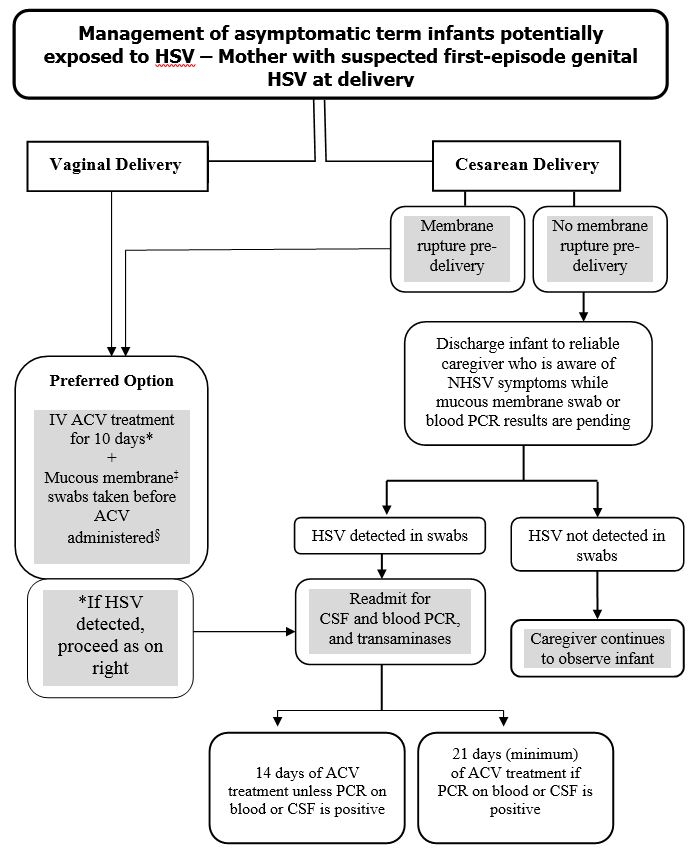
Maternal strategies and obstetric counseling
Pregnant people should tell their providers about any history of HSV. Management decisions—like the choice of delivery route—depend on whether active genital lesions are present at delivery and the timing of maternal infection. Antiviral suppressive therapy in the last weeks of pregnancy can reduce the chance of active lesions at delivery and is commonly discussed with obstetric teams in those with recurrent genital HSV. There is no widely available vaccine for HSV at this time; therefore counseling and prevention are still critical.
If You Suspect Exposure: What to Do Now
Immediate steps
If a newborn has had contact with someone who had a visible cold sore or possible prodromal symptoms, parents should:
- Call the pediatrician right away and describe the exposure and any symptoms the baby has, even if they seem mild.
- Watch closely for early signs—fever, poor feeding, irritability, or any neurologic change.
- Seek emergency care if the infant has a fever, is unusually sleepy, stiff, floppy, or has a seizure.
Clinicians may decide to test the baby and, depending on timing and symptoms, start empiric antiviral therapy. Because antiviral treatment is most effective when given early, erring on the side of caution is often justified.
Administering acyclovir injection—an urgent intervention when HSV encephalitis is suspected
Understanding Risk: How Common—and How Preventable—Is This?
Neonatal HSV is uncommon compared with other pediatric infections, but it carries high morbidity and mortality if it reaches the brain and is untreated. The vast majority of cold-sore episodes in adults never cause harm to infants—if appropriate precautions are taken. However, because a single exposure can be devastating in a neonate, prevention efforts focus on minimizing any avoidable contact during the newborn period.
Emotional and Ethical Dimensions
When an infant becomes ill after contact with a loved one, families experience complex emotions—grief, anger, and overwhelming guilt. Blaming a visitor or relative is natural but rarely productive. Public health messaging should balance truth with compassion: encourage candid discussion of symptoms before visitation, normalize declining visits when someone is unwell, and emphasize support for grieving families. Healthcare providers can help by offering nonjudgmental explanations and clear steps to reduce future risk.
What Pediatricians and Hospitals Do Differently
Hospitals and neonatal units have protocols to reduce risk: screening for active lesions, limiting visitors with symptoms, strict hand hygiene policies, and staff education about HSV. In babies who are ill, pediatric teams use early diagnostic tools, begin empiric antivirals quickly, and coordinate multidisciplinary care—including neurology, infectious disease, and developmental specialists—for survivors.
A note on breastfeeding
Breastfeeding is usually encouraged and safe when there are no breast lesions. If a lactating parent has a herpetic lesion on the breast, direct breastfeeding from the affected breast is generally avoided until the lesion resolves; pumping and feeding after careful hygiene and guidance from the infant’s medical team may be recommended.
Long-term Follow-up and Support
Surviving HSV encephalitis does not always mean a full return to baseline. Many infants require ongoing developmental assessments, therapies (physical, occupational, speech), and sometimes special education services as they grow. Early intervention programs improve outcomes, so timely referral is part of the post-discharge plan. Families may also benefit from counseling and support groups to cope with the emotional aftermath.
Practical FAQs for New Parents
Can I kiss my baby if I have a cold sore?
No—do not kiss the baby on the mouth, lips, or face if you have an active cold sore. Kissing on the top of the head is less risky but still discouraged if a lesion is present or you feel a prodrome.
If someone had a cold sore a week ago, are they still risky?
Viral shedding typically decreases as lesions heal, but some residual risk can remain. As a precaution, avoid close face-to-face contact until the lesion is fully resolved.
Is there a vaccine for HSV?
Currently, there is no widely available vaccine to prevent HSV. Research continues, but prevention today relies on behavior, counseling, and obstetric care.
Conclusion: Small Behaviors, Big Consequences
The story of one infant’s HSV encephalitis underscores a simple but profound truth: everyday actions have outsized effects around newborns. A kiss, a touch, an overlooked symptom—each can be the axis on which a family’s future pivots. The good news is that most of these risks are controllable with awareness, clear rules for visitors, and early medical attention when exposure or symptoms occur. For pediatricians, obstetricians, and families, the task is not to spread fear but to foster informed caution: protect newborns with simple habits, and trust clinicians to act fast if danger appears.
Protecting newborns from HSV encephalitis starts with awareness and preventive measures
- HSV can be transmitted to newborns from people with oral cold sores; postnatal exposure is a preventable risk.
- Early signs of neonatal HSV may be subtle; fever, poor feeding, irritability, and seizures warrant urgent evaluation.
- Empiric intravenous acyclovir is lifesaving and should be initiated promptly when HSV encephalitis is suspected.
- Practical prevention—no kissing on the mouth, strict hand hygiene, and asking symptomatic visitors to stay away—dramatically reduces risk.
- Survivors may need long-term developmental care; early intervention improves outcomes.
If you are a caregiver concerned about HSV exposure in a newborn, contact your pediatrician or emergency services immediately. Rapid evaluation can change outcomes.