Children's Eyes Reveal Early Clues to Depression
When clinicians talk about searching for early signs of depression in children, they typically think about mood changes, sleep problems, appetite shifts and behavior. But over the past decade a quieter, more objective source of information has been emerging: the eyes. Recent work by neuroscientists, pediatric psychiatrists and vision researchers suggests that small differences in how children look—how their pupils respond to light, where their gaze lingers, how often they blink—may offer an early, noninvasive clue to developing mood disorders. That discovery could change how we screen, monitor and ultimately prevent depression, but it also raises challenging questions about privacy, consent and the limits of prediction in young lives.
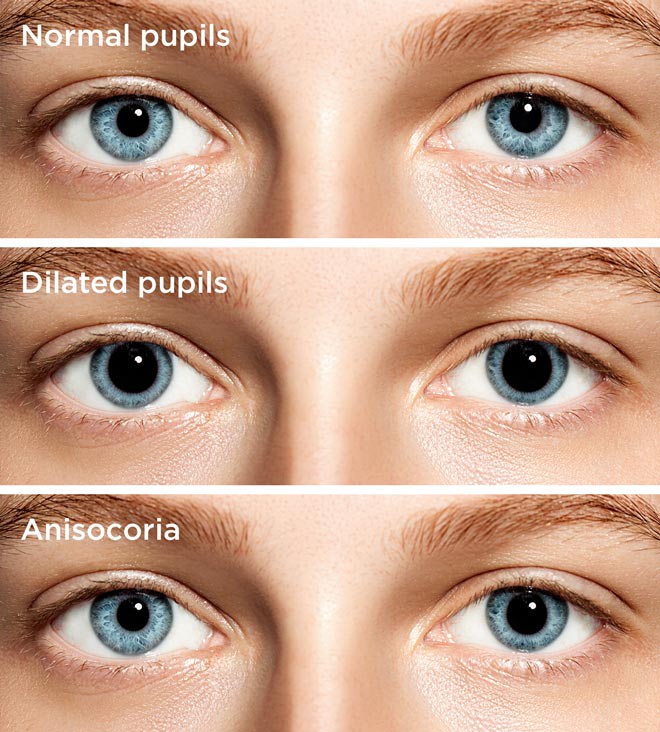
pupil dilation child depression
THE NEW WINDOW: WHY EYES MATTER
Biology on display
The human eye is more than a camera. It is tightly linked to brain systems that regulate attention, arousal and emotion. Pupil size is controlled by autonomic circuits that reflect sympathetic and parasympathetic balance; gaze and saccades are coordinated by cortical and subcortical regions involved in attention and salience; the retina and optic nerve are extensions of central nervous tissue and may reveal neuroinflammatory and metabolic signals. Because these signals are measurable with cameras, eye trackers and retinal imaging tools, researchers can capture objective markers that complement subjective symptom reports in children who may not yet be able to name or describe how they feel.

eye tracking pediatric screening
The promise of early, objective indicators
Subjective screening methods—questionnaires and interviews—are essential but limited. They depend on a child's insight and willingness to report, and on parents' observations. Objective eye-based markers could be used to flag children who benefit from more thorough assessment, to monitor response to treatment, and to study biological mechanisms before full-blown clinical depression appears. For public health systems, a visual screening done in a pediatric clinic or classroom could be faster and less stigmatizing than a mental-health checkup.

retinal imaging children neuroscience
WHAT RESEARCH IS FINDING
Pupil reactions and autonomic signals
Studies have observed that children at higher risk for mood disorders often show subtle but consistent differences in pupil dynamics—diminished dilation to emotional stimuli, slower reactivity to light changes, or a reduced range of pupillary oscillation. Because pupil behavior indexes autonomic nervous system activity, these findings suggest that early dysregulation of arousal and stress responsiveness could be measurable long before diagnostic criteria for depression are met.
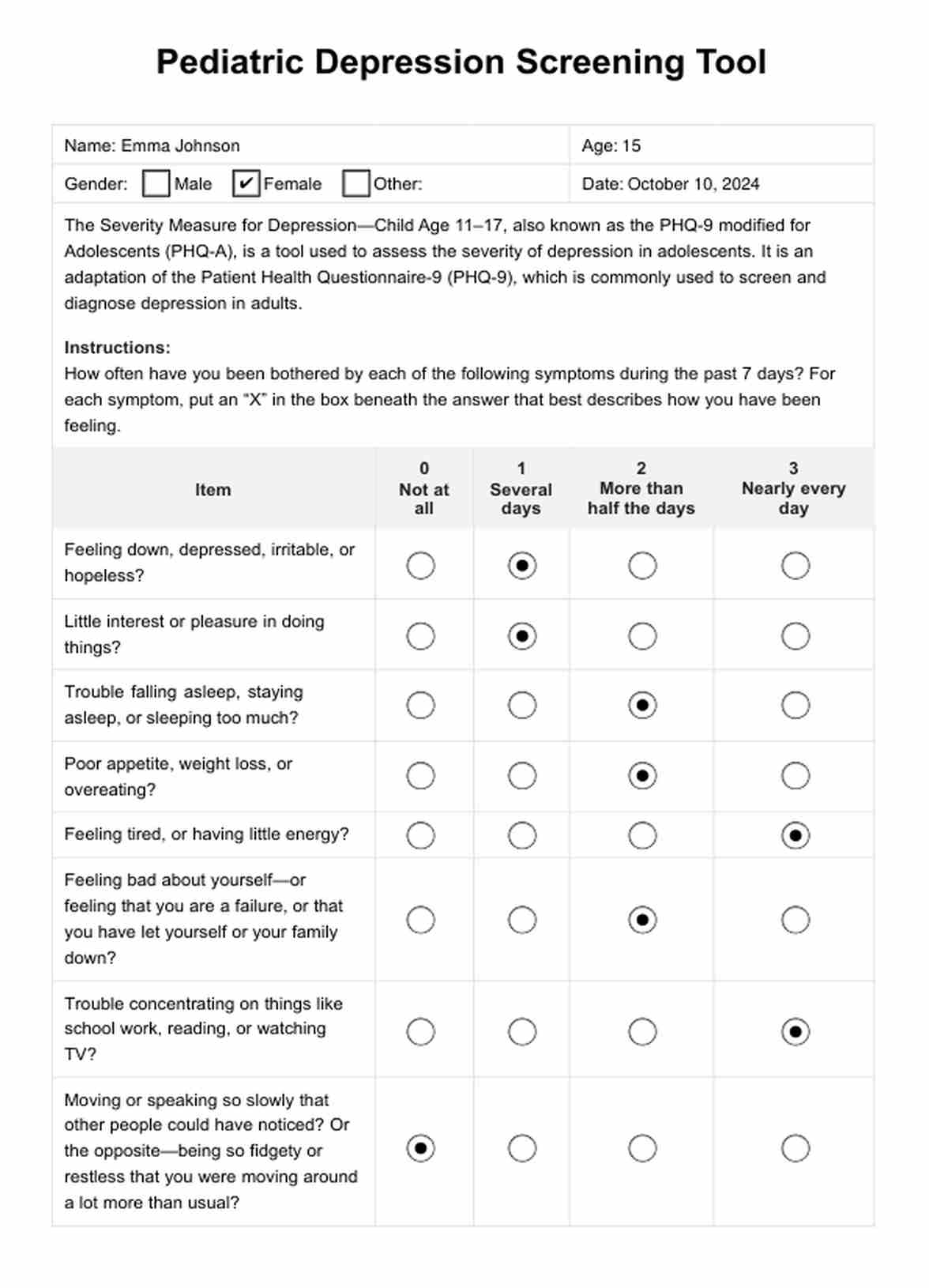
child mental health screening
Gaze patterns, attention and negative bias
Another line of work looks at where children direct their eyes. Children with early depressive tendencies frequently show an attentional bias away from positive social cues and toward neutral or negative faces in controlled tasks. In short, their gaze lingers less on smiling faces and more on ambiguous expressions. These micro-patterns are subtle but replicable with eye-tracking technology, and they link closely to cognitive models of depression that emphasize negative information processing.
pediatric depression biomarkers eyes
Blink rate, saccades, and processing speed
Blinking and saccadic movements offer additional insights. Changes in spontaneous blink rate can relate to dopamine function; slower or more erratic saccades may reflect altered cortical control. In children at risk for depression, researchers have reported altered blink and saccade patterns during tasks requiring emotional discrimination, suggesting early differences in reward processing and executive control.
stress cortisol child eyes
Retinal signs and neuroinflammation
The retina is a direct extension of the brain's central nervous system, and retinal imaging has revealed subtle vascular and structural markers associated with adult psychiatric illnesses in some studies. In children, exploratory work suggests that retinal thickness, microvascular patterns and optic nerve head characteristics could correlate with developmental stressors and inflammatory signals linked to mood dysregulation.
'The eye gives us a fast, objective shorthand for brain states that used to require invasive or costly tests.'
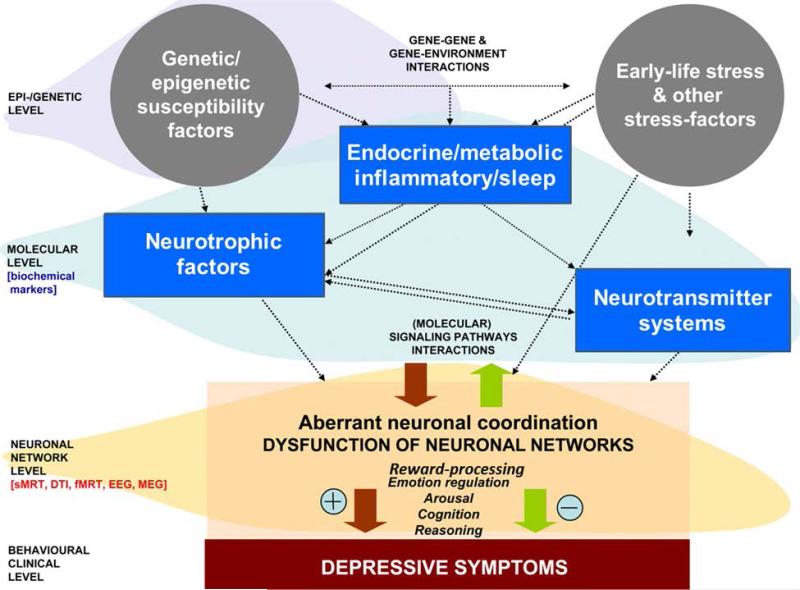
HOW EYE SIGNALS CONNECT TO BIOLOGY
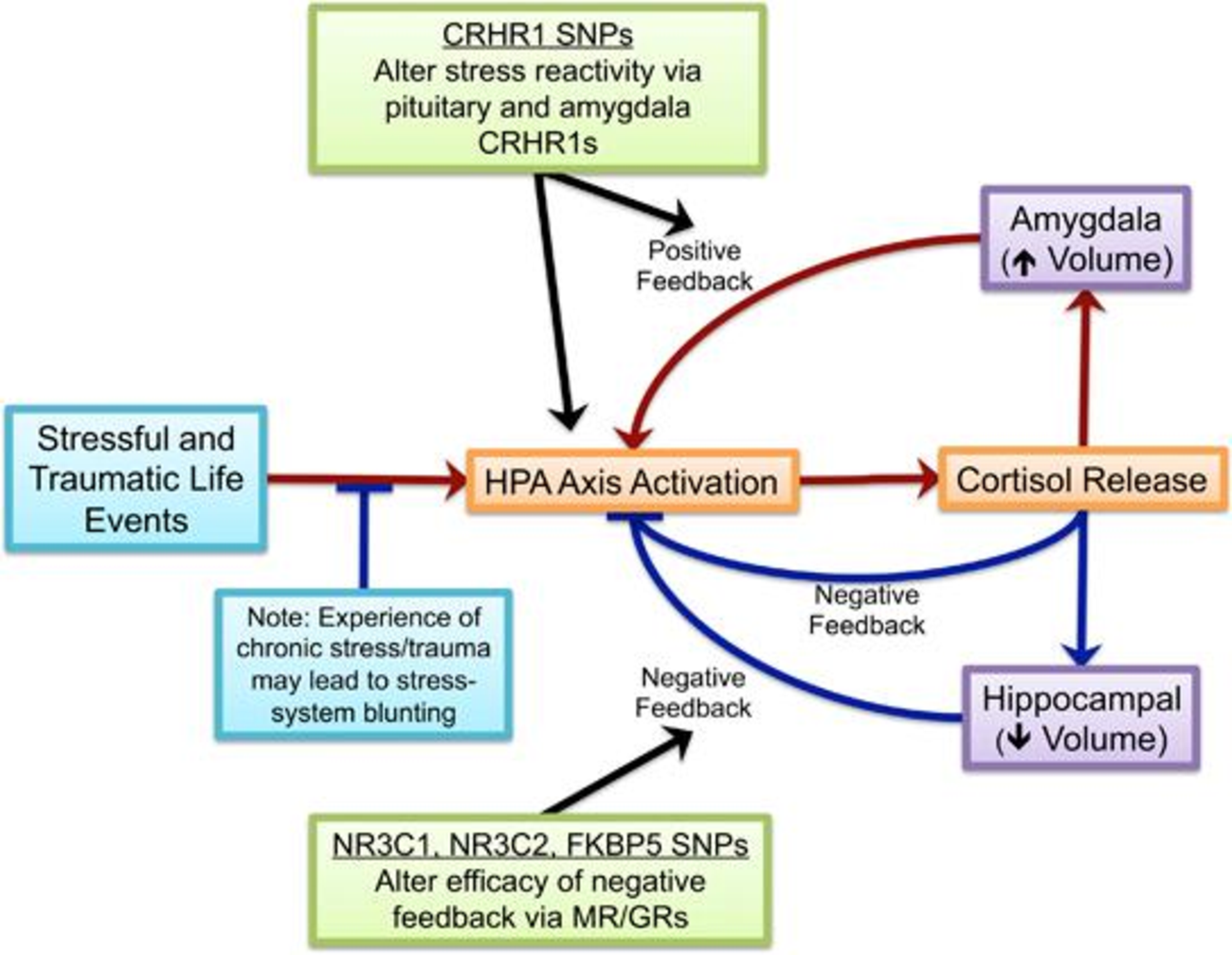
Stress systems and HPA axis
One plausible pathway connecting eye markers to depression risk is stress physiology. Chronic early stress alters hypothalamic–pituitary–adrenal (HPA) axis functioning and sympathetic tone—changes that can be mirrored in pupil responses and baseline arousal. In essence, a child's eye responses may be a downstream readout of prolonged stress exposure and the body's shifting balance between fight-or-flight and rest-and-digest systems.
HPA axis child stress
Neurotransmitters and reward circuitry
Differences in blink rate and gaze allocation are tied to dopamine and other neuromodulators that regulate reward sensitivity. A child whose gaze fails to linger on social rewards or whose blink patterns reflect reduced dopaminergic tone may be showing an early biological expression of anhedonia—the diminished capacity to experience pleasure—that is central to depression.
Inflammation, sleep and circadian rhythms
Emerging evidence links low-grade inflammation and disrupted sleep with mood disorders. Retinal microvasculature and circadian-linked pupil rhythms could therefore be indirect indicators of systemic inflammation or sleep–wake dysregulation in children at risk. Because the eye participates in circadian signaling through intrinsically photosensitive retinal ganglion cells, alterations in light responsiveness can also reflect circadian misalignment—a known contributor to mood problems.
PRACTICAL APPLICATIONS AND LIMITATIONS
From research to screening
Translating eye-based markers into clinical tools requires careful validation. The most realistic near-term applications are adjunctive screening tools in pediatric clinics or school-based programs: a brief eye-tracking and pupillometry session added to routine well-child checks could generate a risk score that prompts follow-up. Similarly, retinal imaging could be incorporated into multidisciplinary assessments when developmental or behavioral concerns arise.
Machine learning and multimodal risk models
Because individual eye markers are noisy and influenced by many factors—lighting, fatigue, medications—researchers are combining multiple signals with demographic, behavioral and genetic data. Machine learning models can weigh patterns across pupil dynamics, gaze metrics, retinal features and questionnaires to produce risk stratifications that outperform any single measure. These multimodal approaches increase predictive power but also amplify ethical and interpretive complexity.
Key limitations to keep in mind
- Non-specificity: Eye markers can signal many conditions—anxiety, ADHD, sleep deprivation—so they are not a diagnostic replacement.
- Developmental variability: Children's visual and attentional systems change rapidly, requiring age-calibrated norms.
- Context dependence: Lighting, time of day, medication, and even excitement about the testing environment affect measures.
- Ethical risks: Predictive labeling of children may stigmatize or lead to unnecessary interventions.
Measurement matters: any screening program must prioritize accuracy, transparency and informed consent.
ETHICAL, SOCIAL AND POLICY CONSIDERATIONS
Consent and assent
Using eye-based screening in children requires robust processes for parental consent and, when appropriate, child assent. The idea of capturing objective biomarkers of mental health raises questions: who sees the results, how are they stored, and how might they be used by schools or insurers? Policies must protect privacy and prevent misuse.
Equity and access
Low-cost eye-tracking tools are becoming available, but unequal access could widen disparities in early detection and care. Any deployment should consider school- and community-based implementation strategies that prioritize underserved populations and avoid reproducing systemic biases.
False positives, labeling and follow-up
Even a modest false-positive rate can have large consequences when screening populations of children. Systems must ensure that positive screens trigger supportive assessment and monitoring rather than immediate medicalization. Interventions should be proportionate, evidence-based and minimally invasive whenever possible.
WHAT FAMILIES AND PROFESSIONALS CAN DO NOW
For parents
Parents should view eye-based findings as one piece of a larger puzzle. If a clinician suggests additional assessment based on an eye screen, ask about what the test measured, what alternative explanations exist, and what the next steps will be. Basic steps—good sleep, routines, safe attachment, and access to supportive counseling—remain the most powerful preventive measures.
For pediatricians and school nurses
Practitioners can stay informed about ongoing validation studies and pilot programs. Where evidence supports it, short objective screens might be added to developmental surveillance—but only with clear referral pathways and safeguards for privacy.
LOOKING AHEAD: RESEARCH PRIORITIES
Longitudinal studies
The critical next step is long-term, population-level research that follows children from early life through adolescence to determine which eye markers reliably predict later depression and under what conditions. These studies need diverse samples and repeated measures to build age-specific norms.
Intervention trials
Researchers must test whether early identification via eye measures leads to better outcomes—does monitoring and low-intensity intervention reduce progression to clinical depression? Evidence of benefit is essential before broad implementation.
Integration with neuroscience
Combining eye markers with neuroimaging, sleep measurement and inflammatory assays will help map causal pathways. Understanding mechanisms increases the chance that early signals become actionable targets for prevention.
Did You Know? The pupil is controlled by both sympathetic and parasympathetic inputs, making it a sensitive, real-time index of stress and arousal.
CONCLUSION
Evidence that children's eyes reveal early clues to depression is one of the most promising developments in child mental health: it offers a noninvasive, scalable way to capture objective signals of risk. But promise is not destiny. Careful validation, ethical guardrails, age-sensitive norms, and a commitment to equitable access are essential. The goal is not to replace clinical judgment or to label children, but to add a sensitive tool to the toolbox—one that helps families and clinicians act earlier, with compassion and precision.
- Objective eye measures—pupil dynamics, gaze, blink rate, retinal features—can signal early risk for depressive trajectories in children.
- These markers are promising for screening and monitoring but are not yet diagnostic and require age-specific validation.
- Ethical implementation must protect privacy, prevent stigma, and ensure equitable access.
- Future research should focus on longitudinal validation, intervention trials, and multimodal integration to turn signals into help.