
A Hidden Vitamin Deficiency That Mimics Normal Aging
It starts slowly: a mislaid word, a walk that leaves your legs trembling, the electric twinge in a fingertip that you shrug off as "getting old." For many people those first hints of change are dismissed. But in a surprising number of cases the culprit is not inevitable aging at all but a common—and treatable—nutrient shortfall: vitamin B12 deficiency. Left unrecognized, it can quietly steal energy, cognition, and nerve function. Recognized early, it's often reversible.
WHY THIS MATTERS
Vitamin B12 (cobalamin) plays a role in DNA synthesis, red blood cell formation, and the maintenance of myelin, the protective sheath that insulates nerves. Deficiency can cause anemia, numbness, difficulty walking, memory problems, mood changes, and fatigue—signs that overlap heavily with conditions associated with aging. That overlap is precisely why B12 deficiency is a clinical masquerader: symptoms are attributed to aging rather than to a correctable medical issue.
WHO IS AT RISK
Older adults
Absorption of B12 from food decreases with age. Many older adults produce less stomach acid and intrinsic factor (a protein required to absorb B12), which raises the likelihood of deficiency even if dietary intake is adequate.
People on restricted diets
Because reliable natural sources of B12 are animal products, strict vegans and some vegetarians are at higher risk unless they use fortified foods or supplements.
People with gastrointestinal surgery or conditions
Surgeries that remove parts of the stomach or small intestine, along with conditions such as celiac disease, Crohn's disease, or bacterial overgrowth, can impair absorption.
Those taking certain medications
Common medications—metformin for diabetes and proton pump inhibitors (PPIs) or H2 blockers for reflux—can reduce B12 absorption when used long term.
WHAT B12 DEFICIENCY LOOKS LIKE
Cognitive and mood changes
Forgetfulness, slowed thinking, difficulty concentrating, and depression are frequent. These complaints often prompt a search for dementia or depression—reasonable avenues—but B12 testing should be part of the evaluation because correction can improve or stabilize mental function.
Neurological signs
Pins-and-needles, burning sensations, numbness, difficulty with balance, and loss of proprioception (the sense of where your limbs are) point to nerve involvement. Unlike purely age-related clumsiness, these signs may progress if untreated and can leave lasting deficits.
Hematologic clues
Macrocytic anemia (larger-than-normal red blood cells), often accompanied by fatigue and pallor, is a classic laboratory clue. But not every person with B12 deficiency has anemia—neurologic symptoms can appear independently.
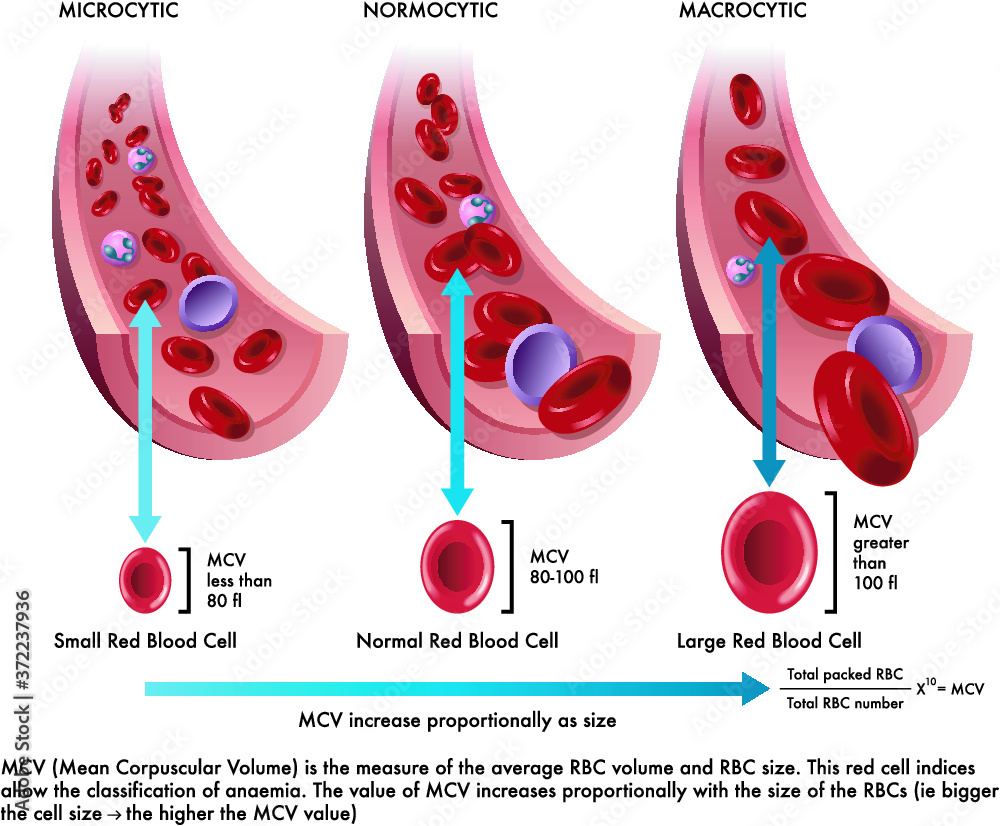
Macrocytic anemia blood cells
'When memory slips and energy dips, think beyond the calendar: nutrient gaps like B12 are fixable.'
HOW B12 IS DIAGNOSED: BEYOND A SINGLE NUMBER
Testing for B12 deficiency is more nuanced than ordering a single serum B12 level. Several labs and clinical clues together give a clearer picture.
Typical tests
Doctors may order:
- Serum B12: A simple screening test but imperfect—values in the low-normal range may still conceal deficiency.
- Methylmalonic acid (MMA): Elevated MMA is a sensitive marker of true B12 deficiency at the cellular level.
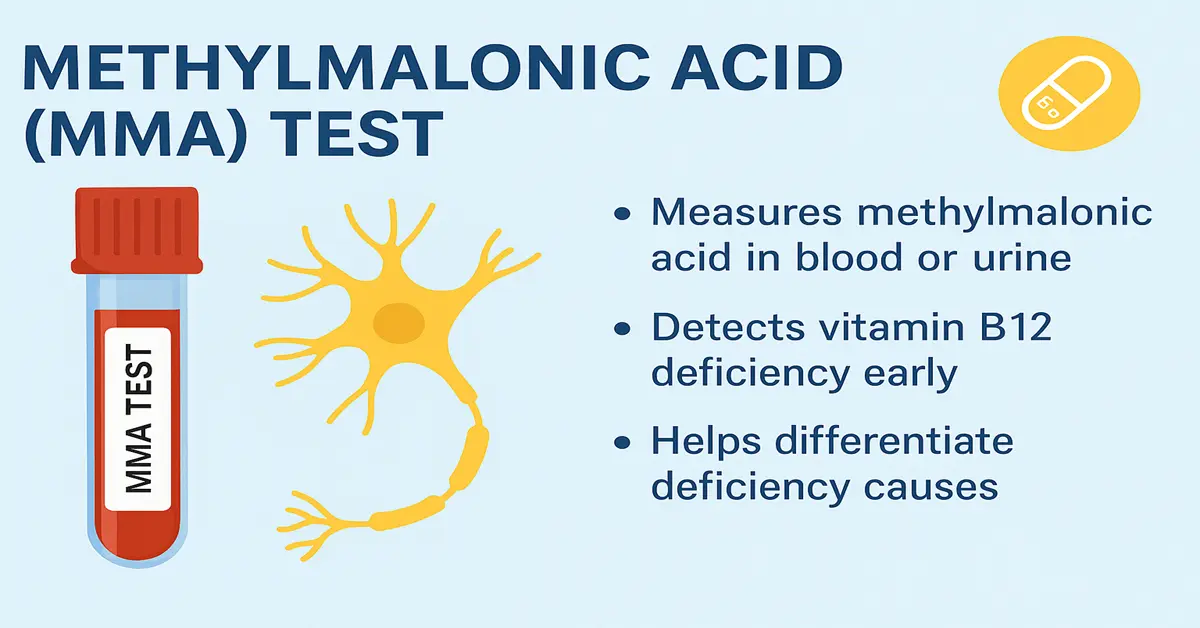
Methylmalonic acid MMA test
- Homocysteine: Can be elevated in B12 deficiency (and in folate deficiency) and offers additional evidence.

Homocysteine blood test
- Complete blood count (CBC): Checks for macrocytic anemia and other hematologic effects.
Putting the pieces together
Because serum B12 can be misleading, clinicians often interpret a low-normal B12 with elevated MMA or homocysteine as active deficiency. Clinical context—neurologic symptoms, medication history, diet, and age—matters equally.
TREATMENT: SIMPLE, OFTEN RAPIDLY EFFECTIVE
Treatment restores levels and often improves symptoms, especially if started early. The route and dose depend on severity and cause.
Oral supplementation
High-dose oral B12 (1,000–2,000 micrograms daily) can correct deficiency even when absorption is reduced, because a small percentage is absorbed passively. For many people with dietary deficiency or mild absorption issues, daily oral supplements are effective and convenient.

Vitamin B12 supplements pills
Intramuscular injections
In cases of severe deficiency, marked neurologic symptoms, or pernicious anemia (where intrinsic factor is absent), injections may be recommended to rapidly restore stores. Protocols vary, but a typical course is frequent injections initially (for example weekly) followed by monthly maintenance.
Vitamin B12 injection medical
Which form of B12?
Two commonly available forms are cyanocobalamin and methylcobalamin. Both raise B12 levels; methylcobalamin is sometimes preferred for neurologic symptoms, though evidence is mixed. Talk with your clinician about the best option for you.
DIETARY SOURCES AND PREVENTION
Preventing deficiency relies on diet, supplementation when needed, and addressing absorption problems.
Food sources
Natural dietary sources include clams, beef liver, sardines, salmon, fortified cereals, dairy, and eggs. For people who avoid animal products, fortified plant milks and cereals plus reliable supplementation are essential.
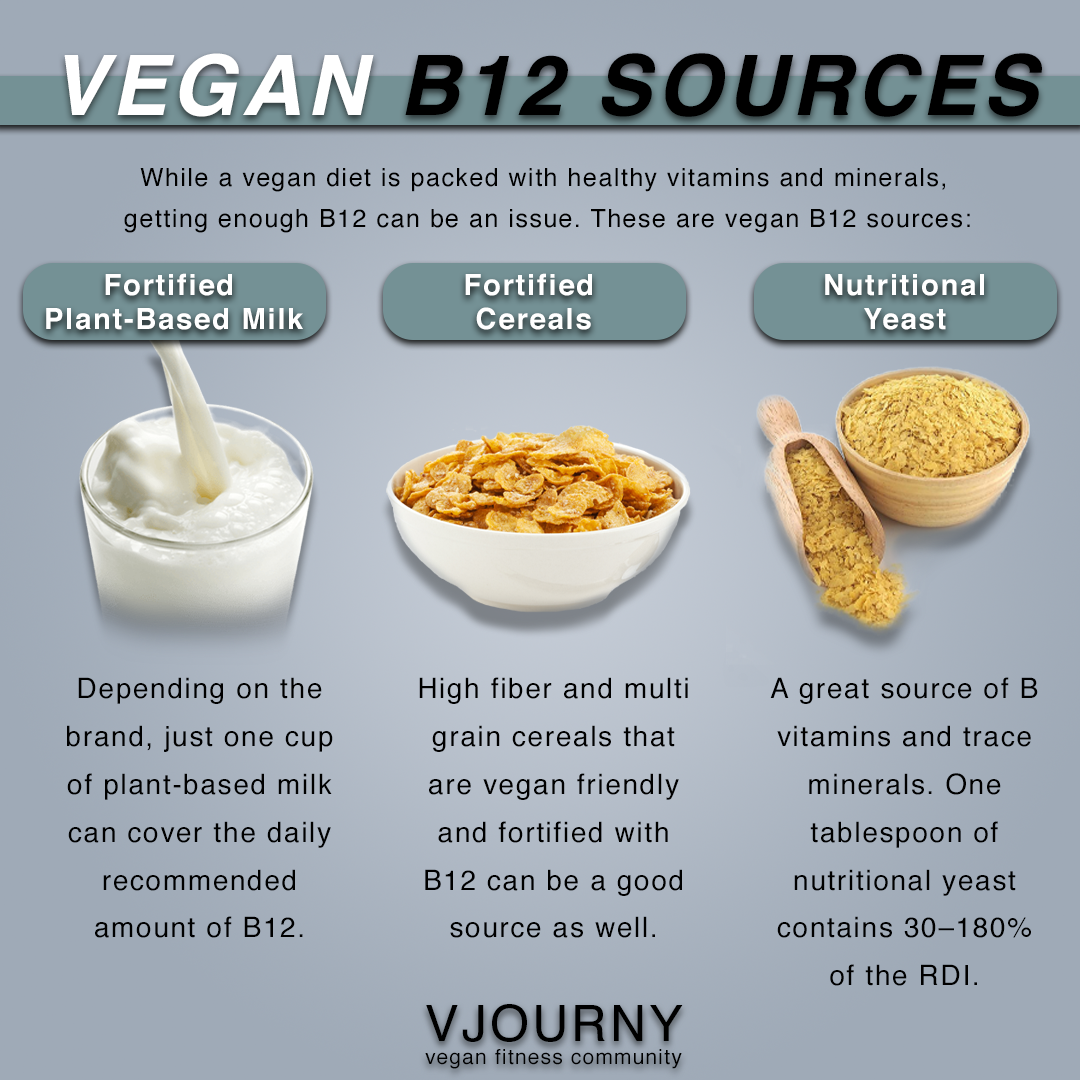
B12 fortified cereals vegan
Lifestyle and medication review
If you take metformin or chronic acid-suppressing medications, ask your clinician about monitoring B12 periodically. Similarly, if you've had bariatric surgery or gastrointestinal disorders, routine checks are prudent.
COMMON QUESTIONS AND MISCONCEPTIONS
Is B12 deficiency reversible?
Often yes—hematologic abnormalities usually correct quickly while neurological recovery may be slower and incomplete if deficiency is prolonged. The sooner treatment begins after symptom onset, the better the chance for full recovery.
Can a normal B12 level rule it out?
No. Normal or low-normal serum B12 does not always rule out deficiency. When clinical suspicion is high, measuring MMA and homocysteine provides greater sensitivity.
Will supplements prevent memory loss?
In people with established B12 deficiency, correcting the deficiency can improve memory and attention. However, taking B12 when levels are already sufficient is unlikely to enhance cognition.
'Diagnosis combines labs and context: numbers rarely tell the whole story.'
A PRACTICAL CHECKLIST: WHEN TO TEST AND WHAT TO ASK
Consider testing if you or a loved one have one or more of the following:
- Persistent fatigue or unexplained anemia.
- New numbness, tingling, or balance problems.
- Worsening memory, word-finding difficulty, or slowed thinking.
- Strict vegan or vegetarian diet without fortified foods or supplements.
- Long-term use of metformin or proton pump inhibitors.
- History of gastric surgery or known malabsorption.
When you see your clinician, mention medications, diet, and any subtle neurologic changes—these details guide which tests to order.
A SIMPLE TABLE: LABS USED TO DIAGNOSE B12 DEFICIENCY
The table below summarizes common tests and what they show.
| Test | What it shows | Notes |
|---|---|---|
| Serum B12 | Amount of B12 in blood | Good screening tool but can be misleading |
| Methylmalonic acid (MMA) | Elevated when cells lack B12 | High sensitivity for deficiency |
| Homocysteine | Raised in B12 or folate deficiency | Supports diagnosis alongside MMA |
RISKS, BENEFITS, AND SUPPLEMENT STRATEGIES
Safety
B12 has a wide safety margin—there's little risk in taking reasonable supplemental doses, though it's best done under medical guidance if you have complex health issues.
- Fast symptom relief for hematologic issues and some neurologic signs.
- Low cost and safe with both oral and injectable options.
- Prevents progression to irreversible nerve damage if treated early.
- Delayed recovery for longstanding neurologic damage.
- Potential need for lifelong therapy in cases like pernicious anemia.
- Variable insurance coverage for injections or specialty labs depending on plans.
WHEN TO SEE A SPECIALIST
Referral to a neurologist or hematologist may be appropriate if neurologic symptoms are severe, the diagnosis is unclear, or the condition fails to improve with initial treatment. A gastroenterologist can help evaluate complex absorption issues.
CONCLUSION
B12 deficiency is common, easily overlooked, and eminently treatable. Because its symptoms overlap with normal aging—cognitive slowing, fatigue, balance trouble—people and clinicians can miss the diagnosis. The remedy is straightforward: test when symptoms or risk factors are present, and treat promptly with supplements or injections. Doing so protects memory, nerves, and daily functioning.
- Vitamin B12 deficiency often mimics normal aging but is treatable and sometimes reversible.
- Testing should include serum B12 and, when indicated, methylmalonic acid and homocysteine.
- High-dose oral B12 or intramuscular injections correct deficiency; early treatment yields the best outcomes.
- People at risk include older adults, vegans, those on metformin or PPIs, and people with GI surgery or disorders.
NEXT STEPS
If you notice persistent fatigue, new numbness, balance issues, or changes in thinking, bring these concerns to your primary care clinician and ask about B12 testing. It's a small step that can make a big difference—sometimes returning months of lost energy, clarity, and mobility.
If you have urgent worsening symptoms—sudden severe weakness, falls, or marked confusion—seek immediate medical care.